TL;DR: In active non-renal SLE, adding the type II anti-CD20 antibody obinutuzumab to standard therapy met its primary endpoint (SRI-4 76.7% vs 53.5% at week 52) and all five key secondary endpoints — delivering both substantial steroid-sparing and a ~40% reduction in flare hazard, and reinforcing that the depth of B-cell depletion is what SLE needs (type II succeeding where rituximab failed).
The Clinical Problem
Despite recent additions to the SLE armamentarium (belimumab, anifrolumab, and voclosporin), many patients with active lupus still live with persistent disease activity, accruing organ damage, treatment-limiting toxicity — chiefly from glucocorticoids — and excess mortality. Two unmet needs dominate long-term care: reducing flares and sparing steroids.
B cells are a compelling target because they generate autoantibodies, present antigen, and secrete cytokines. Yet rituximab (a type I anti-CD20 antibody) failed in its pivotal SLE and lupus nephritis trials. A leading explanation is that active SLE requires deeper B-cell depletion than rituximab reliably delivers.
Obinutuzumab is a glycoengineered type II anti-CD20 monoclonal antibody. Compared with type I agents, it achieves more potent depletion through enhanced FcγRIIIa binding, greater direct cell death, and stronger antibody-dependent cellular cytotoxicity/phagocytosis, with less reliance on complement. It is already approved for lupus nephritis (on the strength of the REGENCY trial). ALLEGORY asked whether that benefit extends to non-renal active SLE.
The Research Question
In adults with active SLE (but without proliferative or membranous lupus nephritis) already on standard therapy, does adding obinutuzumab improve disease activity at week 52 versus placebo?
How the Study Was Designed
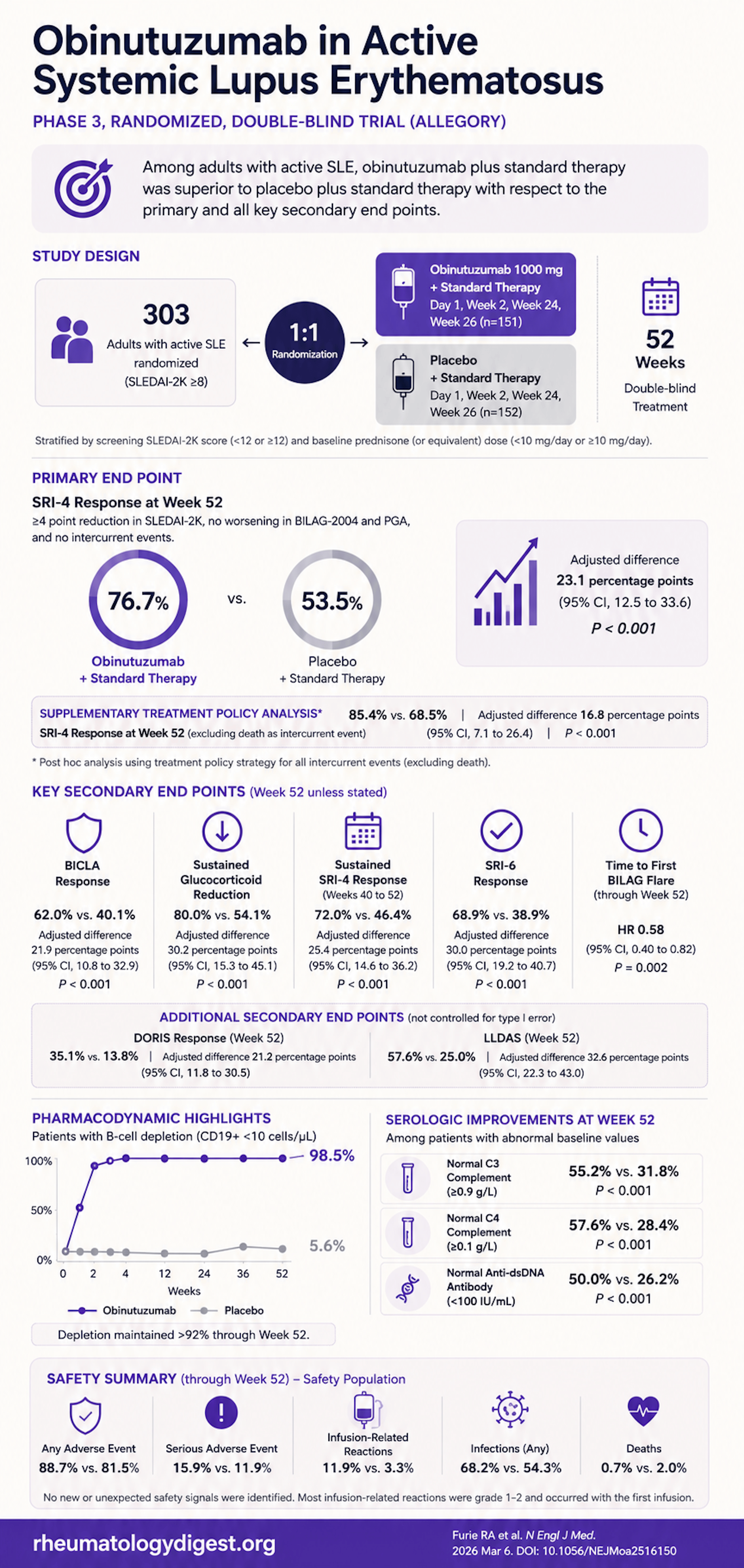
- Design: Phase 3, double-blind, placebo-controlled, 14 countries, 1:1 randomisation to obinutuzumab 1000 mg or placebo, given on day 1 and weeks 2, 24, and 26 — a two-cycle regimen — on top of standard therapy. All received premedication (IV methylprednisolone 80 mg, acetaminophen, diphenhydramine).
- Key entry criteria: Age 18–75; 2019 EULAR/ACR criteria; SLEDAI-2K ≥8 (excluding alopecia/headache/fever points); ≥1 BILAG-2004 domain A or ≥2 domain B; PGA ≥1.0; serologic activity (ANA ≥1:80, or anti-dsDNA ≥100, or anti-Sm ≥100) plus low complement.
- Notable exclusions: proliferative/membranous LN, UPCR >3.5, severe active CNS lupus, and recent anti-CD19/CD20 exposure with depleted B cells — i.e., a non-renal, non-neurologic SLE population.
- Steroid protocol: Patients on >5 mg/day prednisone with improving/stable disease were required to attempt tapering to ≤5 mg/day before week 40 — an important design feature that makes the steroid-sparing endpoint credible.
- Primary endpoint: SRI-4 response at week 52 (a composite: ≥4-point SLEDAI-2K fall, no BILAG/PGA worsening, and no intercurrent events — with intercurrent events counted as non-response under a strict “composite variable” estimand).
- Five key secondary endpoints (hierarchically tested, type-I-error controlled): BICLA response; sustained steroid reduction to ≤7.5 mg/day (wk 40–52, among those on ≥10 mg at baseline); sustained SRI-4 (wk 40–52); SRI-6; and time to first BILAG flare.
- Power: 300 patients gave >90% power to detect a 20-point difference (assumed 55% vs 35%).
- A methodological nuance worth noting: because the strict primary estimand penalises intercurrent events as non-response, the investigators also ran (at editors’ request) a treatment-policy analysis that ignores intercurrent events — useful for judging the “true” pharmacologic effect.
The Results
Population: 690 screened → 303 randomised (151 obinutuzumab, 152 placebo). Genuinely diverse — ~29% American Indian/Alaska Native, ~50–57% Hispanic/Latino, ~15% Black. Mean SLEDAI-2K ~13 (moderate-to-high); disease was predominantly mucocutaneous and musculoskeletal. Notably fewer obinutuzumab patients discontinued (4.6% vs 10.5%).
Primary endpoint — SRI-4 at week 52:
- 76.7% vs 53.5%; adjusted difference +23.1 points (95% CI 12.5–33.6; P<0.001).
- Treatment-policy analysis (intercurrent events not penalised): 85.4% vs 68.5% (+16.8; CI 7.1–26.4). The high placebo rate reflects the strict primary estimand — the drug effect is robust either way.
All five key secondary endpoints were met, in hierarchical order:
| Endpoint | Obinutuzumab | Placebo | Effect |
|---|---|---|---|
| BICLA response (wk 52) | 62.0% | 40.1% | +21.9 pts |
| Steroid ≤7.5 mg sustained (wk 40–52)* | 80.0% | 54.1% | +30.2 pts |
| Sustained SRI-4 (wk 40–52) | 72.0% | 46.4% | +25.4 pts |
| SRI-6 (wk 52) | 68.9% | 38.9% | +30.0 pts |
| Time to first BILAG flare | 33.8% flared | 48.7% flared | HR 0.58 (0.40–0.82) |
All P<0.001 except flare, P=0.002; steroid endpoint assessed in those on ≥10 mg/day at baseline.
Deeper-remission endpoints (not type-I-error controlled, but striking):
- DORIS remission: 35.1% vs 13.8%.
- LLDAS: 57.6% vs 25.0%.
Mechanistic/serologic:
- Rapid, near-complete B-cell depletion — 98.5% depleted by week 2, sustained >92% through week 52.
- Higher rates of C3, C4, and anti-dsDNA normalisation than placebo.
- SLEDAI-2K curves separated from week 24 onward.
Safety:
- Adverse events 88.7% vs 81.5%; serious AEs 15.9% vs 11.9%; grade ≥3 AEs 16.6% vs 13.9%.
- Infections more common (68.2% vs 54.3%; serious infection 8.6% vs 4.6%); most frequent serious infection pneumonia (2.0%).
- Infusion-related reactions 11.9% vs 3.3% (mostly grade 1–2, first infusion).
- Drug-related neutropenia in 7 patients (including 3 grade 3), all resolving (~35 days).
- Deaths: 1 (0.7%) obinutuzumab (soft-tissue infection + pneumonia) vs 3 (2.0%) placebo.
- No hepatitis B reactivation, no PML, IgG maintained in normal range.
Study Limitations
- Excluded the sickest renal and CNS patients (proliferative/membranous LN, severe CNS lupus) — standard for SLE trials but limits generalisability to exactly those high-stakes scenarios.
- 52-week horizon — no conclusions on long-term efficacy or safety, or on durability of the two-cycle dosing.
- No tissue sampling — so whether tissue-level B-cell depletion drove the clinical responses cannot be confirmed from this trial (the authors lean on REGENCY and THEORY tissue data to argue it does).
- High placebo SRI-4 response under the strict estimand complicates cross-trial comparison.
- Higher infection burden requires ongoing vigilance, and neutropenia is a recognised class effect.
How This Study Adds to Practice
- It extends obinutuzumab’s evidence base from lupus nephritis (REGENCY) to active non-renal SLE, and did so in a population with higher baseline disease activity than many prior SLE trials — yet still achieved notably high remission (DORIS) and LLDAS rates.
- It hits both of SLE’s central unmet needs simultaneously: steroid-sparing (80% vs 54% tapered to ≤7.5 mg) and flare reduction (HR 0.58) — the two outcomes that most drive long-term damage.
- It strengthens the broader thesis that depth of B-cell depletion matters in SLE: a type II anti-CD20 succeeds where type I (rituximab) failed, consistent with the deep-depletion signal from CD19 CAR-T. This reframes rituximab’s failure as a depletion problem, not a refutation of the B-cell hypothesis.
- Practically, the two-cycle IV regimen (four infusions over ~6 months) is a manageable schedule that fits treat-to-target, low-steroid management paradigms now emphasised in ACR/EULAR guidance.
Final Take-Aways
- Obinutuzumab met its primary endpoint and all five key secondary endpoints in active non-renal SLE — SRI-4 76.7% vs 53.5% at week 52.
- Two of the highest-value outcomes were achieved together: substantial steroid-sparing and a ~40% reduction in flare hazard.
- Depletion was fast and deep (98.5% by week 2, >92% sustained), reinforcing that type II > type I anti-CD20 for the depletion SLE seems to require.
- Remission-level responses (DORIS 35% vs 14%, LLDAS 58% vs 25%) are impressive given the higher baseline activity, though these weren’t type-I-error controlled.
- Safety was acceptable and consistent with the known profile — more infections and infusion reactions, manageable neutropenia, and fewer deaths than placebo — but the population excluded severe renal/CNS disease and follow-up was only 1 year.
- Positioning: a strong candidate for moderate-to-severe active SLE inadequately controlled on standard therapy, especially where steroid-sparing and flare prevention are priorities — pending longer-term and tissue-level data.