TL;DR: In the VALOR trial, brepocitinib 30 mg daily — a selective TYK2–JAK1 inhibitor — significantly improved composite disease activity, skin involvement, and muscle strength in refractory dermatomyositis, with 42% of treated patients achieving complete steroid discontinuation, marking the first oral targeted therapy to succeed in a phase 3 RCT in this disease.
The Clinical Problem
Dermatomyositis (DM) is a chronic, multisystem autoimmune disease affecting muscles, skin, lungs, joints, heart, and GI tract. Despite decades of using glucocorticoids, conventional DMARDs (MTX, MMF, AZA), and IVIG, outcomes remain unsatisfactory:
- Incomplete efficacy in a substantial proportion of patients
- Cumulative steroid toxicity (infection, osteoporosis, diabetes, CV disease, steroid myopathy)
- Persistent skin disease even when muscle disease responds
- Substantial morbidity, disability, and impaired quality of life
The cytokine basis of DM is now well established. Type I and II interferons, IL-6, IL-12, and IL-23 drive immunopathogenesis. TYK2 and JAK1 are the key intracellular signal transducers for these cytokines, making this dyad an attractive therapeutic target.
Brepocitinib is a first-in-class, oral, selective TYK2–JAK1 inhibitor. Unlike pan-JAK inhibitors, it spares JAK2 and JAK3, theoretically offering a more favourable safety profile while still blocking IFN-driven inflammation.
The Research Question
Does once-daily oral brepocitinib (30 mg or 15 mg) improve disease activity in adults with treatment-refractory dermatomyositis, compared with placebo, over 52 weeks?
How the Study Was Designed
Design: Phase 3, multicentre, double-blind, randomised, placebo-controlled trial (VALOR; NCT05437263), funded by Priovant Therapeutics. Conducted at 90 sites across 20 countries between October 2022 and June 2024.
Population (n = 241): Adults 18–75 years with:
- 2017 EULAR/ACR criteria for definite or probable IIM with DM subclassification
- Active muscle disease: MMT-8 score 80–142 (out of 150; lower = weaker)
- Active skin disease: CDASI-A ≥ 6 (out of 100; higher = more active)
- Inadequate response to at least one prior therapy (steroids, conventional DMARDs, or IVIG)
Randomisation: 1:1:1 to brepocitinib 30 mg, brepocitinib 15 mg, or placebo, once daily for 52 weeks. Stratified by Physician Global Assessment (PhGA-VAS 0–4.9 vs 5.0–10 cm).
Background therapy rules:
- One antimalarial and/or one conventional DMARD continued at stable dose
- Steroids tapered to ≤ 20 mg prednisone equivalent/day pre-randomisation
- A brief steroid pulse (up to 60 mg/day) permitted weeks 1–12
- Protocol-defined steroid taper from week 12, with goal of ≤ 5 mg/day by week 36
Primary endpoint: Mean Total Improvement Score (TIS) at week 52. The TIS is a validated weighted composite (0–100) integrating six core measures of myositis activity (PhGA, patient global, MMT-8, HAQ, muscle enzymes, extramuscular disease).
Nine multiplicity-controlled key secondary endpoints:
- Change in CDASI-A at week 52
- DMOMS score at week 52 (newer skin + muscle composite)
- Proportion with TIS ≥ 40 (moderate improvement)
- Time to sustained TIS ≥ 40 (two consecutive visits)
- TIS ≥ 40 combined with steroid dose ≤ 2.5 mg/day at weeks 48–52
- Clinically meaningful skin response (≥ 40% AND ≥ 4-point CDASI-A reduction)
- TIS ≥ 60 (major improvement)
- Change in HAQ-DI at week 52
- Change in CDASI-A at week 4 (early response)
Exploratory: MMT-8 change and skin clinical remission (CDASI-A ≤ 5).
Statistical approach:
- Sample size 225 (75/arm) gave 98% power at α = 0.05 (two-sided) to detect a 15-point TIS difference (assumed SD 23)
- ITT analysis; ANCOVA with baseline PhGA and background therapy as covariates
- Hierarchical stepwise testing: 30 mg first vs placebo; only if positive would 15 mg vs placebo be formally tested
- Hybrid estimand: death/rescue medication imputed as non-response; early discontinuation handled by LOCF
The Results
Baseline characteristics: Mean age 50.6 years, 77.6% women, predominantly White (71%) with 24% Hispanic/Latino. The cohort was unequivocally treatment-refractory:
- 92.9% on at least one DM-directed systemic therapy
- 75.5% on glucocorticoids (mean prednisone equivalent 11.4 ± 6.0 mg/day)
- 81.3% on ≥ 2 systemic therapies concurrently
- 25.3% previously exposed to IVIG; 10.8% to rituximab; 7.1% to cyclophosphamide
- Mean CDASI-A 19.8, mean MMT-8 122.6
- ILD in 19.5%; prior neoplasm in 14.1%; ≥ 1 CV risk factor in 64.7%
Trial retention:
- 87.1% completed 52 weeks
- Discontinuation: placebo 25% vs brepocitinib 30 mg 11%
- Rescue medication used: placebo 30% vs brepocitinib 30 mg 15%
Primary Endpoint
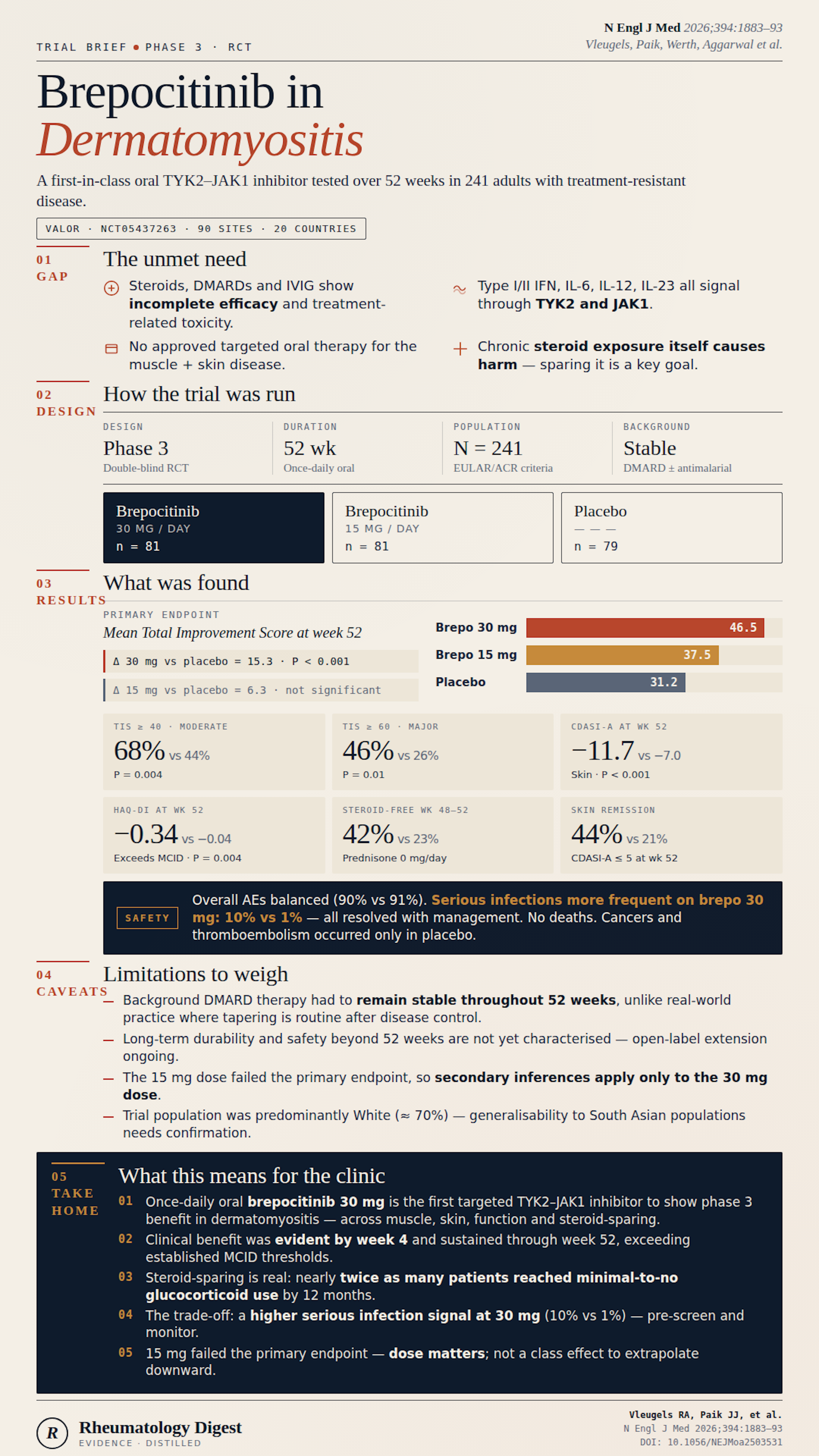
Mean TIS at week 52:
- Brepocitinib 30 mg → 46.5
- Brepocitinib 15 mg → 37.5
- Placebo → 31.2
30 mg vs placebo: LS-mean difference 15.3 points (95% CI 6.7–24.0), P < 0.001
15 mg vs placebo: difference 6.3 (95% CI −2.4 to 14.9) — not significant; per hierarchical testing, no further hypothesis testing for the 15 mg arm.
Key Secondary Endpoints (Brepocitinib 30 mg vs Placebo)
All nine were positive:
- TIS ≥ 40 (moderate response): 68% vs 44% (risk difference 22.2 pp; P = 0.004)
- TIS ≥ 60 (major response): 46% vs 26% (RD 19.5 pp; P = 0.01)
- TIS ≥ 40 + steroids ≤ 2.5 mg/day at wk 48–52: 54% vs 27% (P < 0.001)
- CDASI-A at week 52: −11.7 vs −7.0 (diff −4.6; P < 0.001)
- CDASI-A at week 4 (early skin response): −6.4 vs −3.5 (diff −3.0; P < 0.001)
- Clinically meaningful skin response: 62% vs 44% (P = 0.04)
- DMOMS at week 52: 57.9 vs 40.5 (diff 17.3; P = 0.001)
- Median time to sustained TIS ≥ 40: 85 days vs 168 days (HR 1.60, 95% CI 1.09–2.33; P = 0.02) — nearly halved
- HAQ-DI change: −0.337 vs −0.042 (diff −0.295; P = 0.004) — exceeds the MCID of 0.22
Steroid Sparing (Among Baseline Steroid Users)
- Tapered to ≤ 2.5 mg/day: 62% (30 mg) vs 34% (placebo)
- Tapered to 0 mg/day: 42% (30 mg) vs 23% (placebo)
So nearly twice as many patients on brepocitinib achieved virtual steroid discontinuation — and this happened alongside (not at the expense of) better disease control.
Exploratory Endpoints
- MMT-8 change: +13.5 (30 mg) vs +8.7 (placebo)
- Skin clinical remission (CDASI-A ≤ 5) in those with baseline moderate-severe skin disease: 44% vs 21%
Safety
Overall adverse event rates were broadly comparable (90% / 86% / 91% across 30 mg / 15 mg / placebo). The standout signal:
| Adverse Event | 30 mg | 15 mg | Placebo |
|---|---|---|---|
| Any serious AE | 16% | 9% | 13% |
| Serious infections | 10% | 2% | 1% |
| Viral reactivation (mostly VZV) | 5% | 2% | 5% |
| Cardiovascular | 1% (1 CVA) | 0 | 3% |
| Thromboembolic | 0 | 0 | 1% (PE) |
| Malignancy | 0 | 0 | 3% (NPC, SCC) |
| ALT/AST ≥ 3× ULN | 1% | 2% | 1% |
Key points:
- No deaths during the trial
- Serious infections resolved with medical management; most patients completed treatment
- Notably, MACE, VTE, and cancers occurred only in placebo arm, likely reflecting baseline DM-associated risk and concurrent steroid exposure rather than drug benefit
- More overall discontinuations due to serious AEs in the placebo group (11%) than brepocitinib groups (6–7%)
Study Limitations
- Mandatory stable background DMARD therapy throughout the trial. In real practice, DMARDs are typically tapered once disease control is achieved. The trial therefore cannot tell us whether brepocitinib could serve as monotherapy. The ongoing 52-week open-label extension is designed to address this.
- No active comparator (e.g., IVIG, rituximab, or another JAKi). We do not yet know where brepocitinib sits in the therapeutic hierarchy.
- Refractory population only — efficacy in treatment-naive or milder disease is untested.
- 52 weeks is short for a chronic disease. Durability of response, long-term infection/malignancy/MACE risk, and effect on damage accrual remain to be characterised.
- Limited ILD population (~20%); the trial was not powered to assess ILD-specific outcomes — a major unmet need in DM.
- Industry-funded, with sponsor involvement in design, analysis, and interpretation.
- No biomarker stratification (e.g., MSA/MAA subgroups such as anti-MDA5, anti-Mi2, anti-TIF1γ, anti-NXP2). Whether response varies by autoantibody phenotype is unknown.
How This Study Adds to Practice
- First successful Phase 3 trial of a targeted oral agent in DM, validating the IFN/TYK2–JAK1 axis as a therapeutic target. Previously, IVIG (ProDERM, NEJM 2022) was the only modern RCT-validated agent.
- Dual benefit on skin AND muscle, which is uncommon — historically, skin disease has been the most refractory domain and often persists after muscle disease responds.
- Rapid onset (week 4 separation on CDASI-A) is clinically meaningful, particularly for patients with severely active, disfiguring cutaneous disease.
- Genuine steroid-sparing effect, with 42% achieving complete steroid discontinuation — directly addressing the most consequential long-term morbidity driver in DM.
- Dose matters: only 30 mg met the primary endpoint. The 15 mg dose was not adequate, suggesting incomplete cytokine pathway blockade at lower exposure.
- The serious infection signal (10% vs 1%) requires vigilance and is consistent with class effects of JAK/TYK2 inhibition. Pre-treatment screening (VZV, HBV, TB) and possibly VZV vaccination strategies will be relevant if approved.
- The absence of MACE, VTE, and malignancy signals in the active arm is reassuring but must be interpreted cautiously given the modest sample size and 52-week duration — the ORAL Surveillance experience with tofacitinib in RA reminds us that such signals can emerge with longer exposure.
Final Take-aways
- In adults with refractory dermatomyositis, brepocitinib 30 mg daily significantly improves a composite myositis index, skin disease, muscle strength, physical function, and steroid burden, with benefits visible by week 4 and sustained at 52 weeks.
- Brepocitinib 15 mg is ineffective for the primary endpoint — the 30 mg dose is the clinically relevant one.
- Steroid sparing is real and substantial — ~40% of treated patients came off steroids entirely. This is arguably the most important practical signal for long-term morbidity reduction.
- Safety trade-off: a 10× increase in serious infections vs placebo. No deaths, no excess MACE/VTE/malignancy in this 52-week dataset, but longer follow-up is essential.
- Open questions: monotherapy potential, comparative efficacy versus IVIG/rituximab, autoantibody-stratified response, ILD outcomes, and long-term safety. The open-label extension will start to fill these gaps.
- Clinical bottom line: if approved, brepocitinib would be the first oral targeted therapy for DM and a potentially major addition to a sparse therapeutic toolkit — especially for patients with refractory skin disease and those struggling to taper steroids.