A detailed summary of the Current Opinion review by Koumpouras & Caricchio (Curr Opin Rheumatol 2026; 38:155–162)
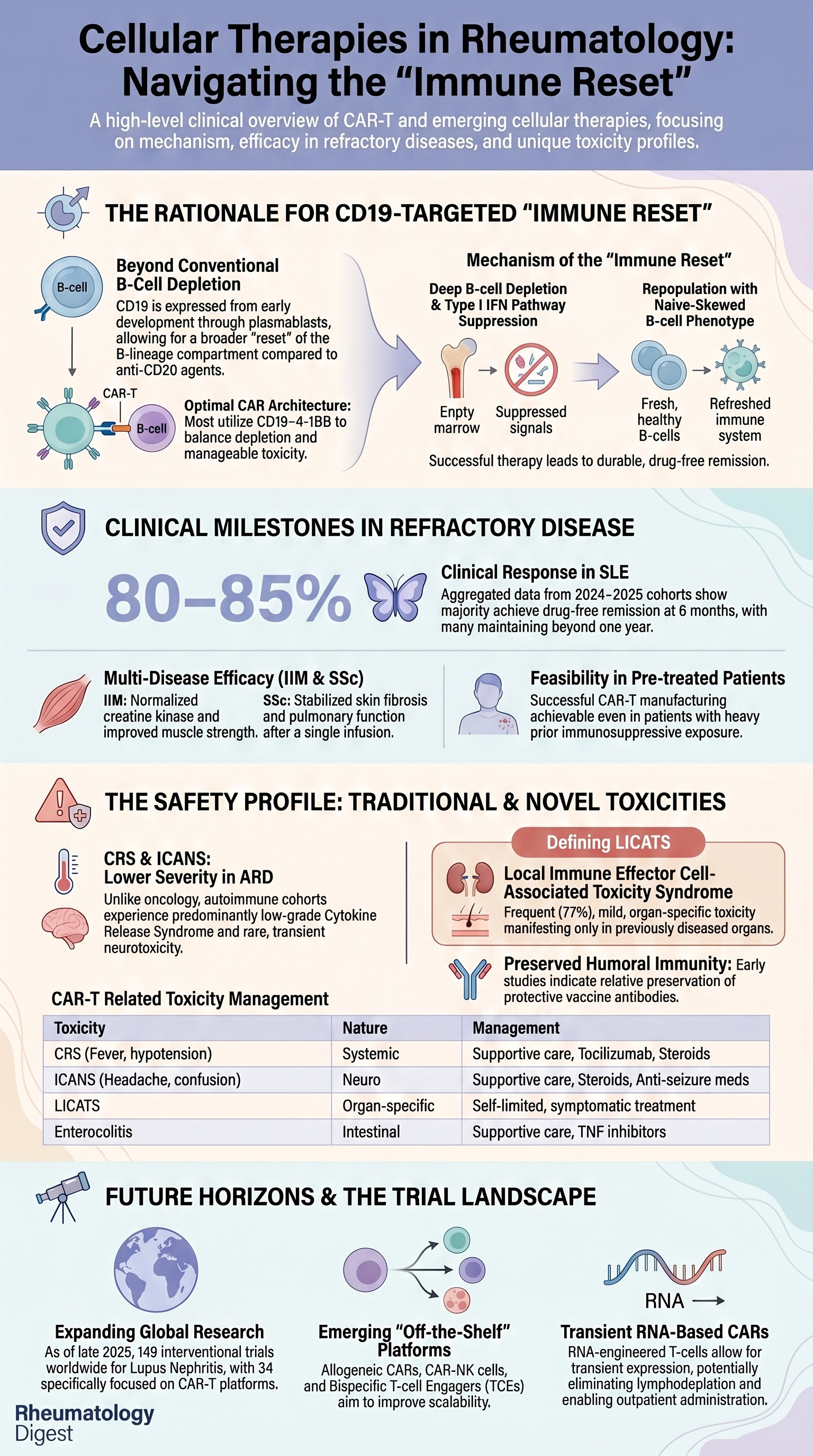
TL;DR: CD19 CAR-T cellular therapy delivers drug-free remission in 80–85% of refractory SLE patients in early-phase trials, with similar signals in IIM and SSc — the first credible attempt at true immunological reset, replacing chronic immunosuppression with a one-and-done intervention.
The Clinical Problem
Despite a steady expansion of the therapeutic armamentarium, systemic lupus erythematosus (SLE), lupus nephritis, idiopathic inflammatory myopathies (IIM), and systemic sclerosis (SSc) still leave a substantial proportion of patients with refractory disease, accumulating organ damage, and steroid-related comorbidity.
Key limitations of current paradigms:
- Conventional immunosuppressants and even newer targeted agents (type I IFN receptor blockade with anifrolumab, BAFF inhibition with belimumab, calcineurin inhibition with voclosporin) improve outcomes but rarely deliver durable, complete renal remission.
- Cumulative glucocorticoid exposure continues to drive damage and comorbidity.
- Attempts to taper immunosuppression in proliferative lupus nephritis are typically thwarted by relapse — reflecting the failure of conventional therapy to truly reset autoimmunity.
- Anti-CD20 antibody-based depletion is incomplete: Phase II/III rituximab trials in SLE missed their primary endpoints; even type II anti-CD20 obinutuzumab (REGENCY trial) gives deeper depletion and better renal responses but seldom produces sustained drug-free remission.
A paradoxical “unmet need amidst an overcrowded pipeline” is now evident — more than 30 active interventional trials are exploring cell-based strategies in lupus nephritis alone (149 trials worldwide in LN, 34 of which are CAR-T trials, per ClinicalTrials.gov, Oct 2025).
What the Paper Explains
This is a narrative review synthesising the rationale, current clinical experience, safety landscape, and emerging platforms for cellular therapy in rheumatic disease. The authors cover six conceptual areas, summarised below.
1. Foundations of Cellular Immunotherapy & CAR Design
- The field grew out of oncology — IL-2-expanded lymphocytes, tumour-infiltrating lymphocytes, then retroviral gene transfer of tumour-reactive receptors into autologous T cells.
- A chimeric antigen receptor (CAR) combines:
- An extracellular single-chain variable fragment (scFv) for antigen recognition
- Intracellular CD3ζ activation domain
- One or more co-stimulatory domains — typically CD28 or 4-1BB
- Design matters:
- CD28-based CARs → brisk expansion, shorter persistence
- 4-1BB-based CARs → slower expansion, longer persistence
- Most autoimmune programmes have therefore converged on CD19–4-1BB architectures, to balance deep B-cell depletion with manageable toxicity.
2. Why CD19 Is a Compelling Target in Autoimmunity
- CD19 spans a broader B-lineage range than CD20 — from pro-B cells through naïve and memory B cells, plasmablasts, and a subset of short-lived plasma cells.
- CD20 is absent from pro-B cells and many antibody-secreting cells.
- CD19-directed CAR-T can therefore reach autoreactive cells in tissue niches or microenvironments that monoclonal antibodies struggle to penetrate.
- Important nuance: In murine SLE models, CD19 CAR-T prolongs survival and prevents glomerulonephritis when depletion is sustained. However, in the Fra2 TG murine model of SSc, deep B-cell depletion did NOT help — it exacerbated disease (Avouac et al., A&R 2024). This is a not-so-obvious cautionary signal that mechanisms beyond simple B-cell depletion may be relevant in SSc.
- Practical feasibility: Leukapheresis and CAR-T manufacturing have proven feasible even in patients on background immunosuppression; ex vivo cytotoxicity of SLE-derived CAR-T products is comparable to that of healthy-donor products.
3. Clinical Experience in SLE, IIM, and SSc
Sequential milestones:
- First case (Mackensen 2022): A young adult with refractory SLE + active lupus nephritis received CD19–4-1BB CAR-T → rapid B-cell depletion → complete clinical and serological remission, drug-free.
- Five-patient series: All achieved DORIS-defined drug-free remission within 3 months, normal complement, minimal/no proteinuria, and B-cell repopulation predominantly with naïve cells — a key feature of “immune reset.”
- Erlangen Phase I/II basket study (n = 24):
- 17 women, 7 men; median age 39 years
- 10 SLE, 9 SSc, 5 IIM
- Median of 4 prior immunosuppressive treatments
- CRS: 18/24 developed CRS — 17 grade 1, 1 grade 2; no higher-grade CRS, no ICANS
- No clinically relevant cytopenia >4 weeks
- One grade 3 event — renal thrombotic microangiopathy with CMV co-infection
- LICATS in 88% (mostly grade 1/2)
- B-cell depletion in all patients
- 6-month efficacy (19/24 patients):
- 7/7 SLE → DORIS remission
- 8/8 SSc → no disease progression
- 4/4 IIM → ACR/EULAR moderate or major response
- All 24 patients discontinued immunosuppression.
- Aggregated 2024–25 reviews: Approximately 80–85% of refractory SLE patients in early-phase CAR-T trials achieve complete clinical response, most in drug-free remission at 6 months, many maintaining remission beyond 1 year.
Subtle caveat highlighted by the authors: In lupus nephritis, persisting proteinuria may reflect chronic damage rather than ongoing activity, which can make complete clinical responses look less impressive than they truly are.
4. Toxicity & Safety — The Distinctive Autoimmune Profile
The toxicity pattern in autoimmune disease differs meaningfully from oncology, where tumour burden drives severity.
Major toxicities (Table 1 of the paper):
- Cytokine Release Syndrome (CRS)
- Systemic inflammatory response — fever, hypotension, organ dysfunction
- Onset 1–7 days post-infusion
- In autoimmune cohorts: predominantly grade 0–1, occasional grade 2
- Management: supportive care, tocilizumab, corticosteroids
- Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS)
- Headache, confusion, seizures
- 1–7 days post-infusion
- Rare in autoimmune cohorts; transient neurocognitive symptoms only
- Not observed in the CASTLE study
- Local Immune Effector Cell-Associated Toxicity Syndrome (LICATS) — newly described entity
- Occurred in 77% of 39 patients (SLE, SSc, IIM)
- 54 events total, distribution:
- Skin — 35%
- Kidneys — 22%
- Musculoskeletal — 19%
- Onset ~10 days post-infusion, during B-cell aplasia
- Resolves in ~11 days, usually without intensive treatment (brief steroids often suffice)
- Crucially: confined to organs previously involved by the underlying autoimmune disease
- No serology of flare, no histological evidence of active autoimmunity in limited biopsies
- Hypothesised to represent a local inflammatory “cleansing” during deep tissue B-cell depletion
- Recognising this is important to avoid inappropriately re-starting immunosuppression
- Immune Effector Cell (IEC)-Associated Enterocolitis
- Diarrhoea, abdominal pain, colitis
- Intra-epithelial lymphocytosis with villous blunting; CAR-T cells confirmed in lamina propria in one myeloma case
- FDA has issued updated black-box warnings in haematologic indications
- Management: supportive care, anti-inflammatories, immunosuppression (TNF inhibitors, integrin blockers)
- Other concerns
- Hypogammaglobulinaemia and infection risk — but early SLE data show preserved pre-existing vaccine titres (consistent with sparing of CD19-negative long-lived plasma cells) and capacity to boost on revaccination
- Class-wide regulatory warnings for secondary T-cell malignancies following BCMA- and CD19-CAR-T in oncology — drives the need for long-term surveillance in autoimmune recipients
Practical bridging note: Gerber et al. (Lupus Sci Med 2025) showed that brief pulse corticosteroids during the immunosuppressive washout period can control severe lupus flares without compromising CAR-T expansion, B-cell depletion, or durable remission — a clinically useful tip.
5. Beyond SLE — Expanding Indications
- Idiopathic Inflammatory Myopathies (IIM, including antisynthetase syndrome):
- CD19 CAR-T used as rescue after multiple failed B-cell-depleting antibodies
- Major gains in muscle strength, CK normalisation, resolution of lung involvement
- Subtle observation: Some patients showed later transient flares attributed to expansion of autoreactive CD8+ effector cells — possibly driven by low-grade LICATS. Highlights the need for T-cell monitoring.
- Systemic Sclerosis (SSc):
- A single infusion can stabilise/improve skin fibrosis, digital ischaemia, and pulmonary function — without ongoing immunosuppression
- Neurologic autoimmunity (not classic rheumatology but conceptually adjacent):
- BCMA- and CD19-CAR-T used in neuromyelitis optica spectrum disorder (NMOSD) and myasthenia gravis → marked reductions in pathogenic autoantibodies, relapse rates, and disability scores. Supports the broader principle that B-lineage-directed cell therapy resets pathogenic humoral immunity across diverse antibody-mediated diseases.
6. Transient and Alternative Effector Platforms
To circumvent the long-term risks of integrating vectors, manufacturing complexity, and lymphodepletion, several alternatives are under development:
- Transient RNA-based CAR-T
- RNA electroporation or mRNA vectors → CAR expression is finite
- In a Phase 1b/2a MG study: ex vivo RNA-engineered BCMA CAR-T allowed patients to remain on baseline immunosuppression, avoided lymphodepleting conditioning, enabled outpatient infusion, with minimal CRS/ICANS
- In a separate study, LNP-encapsulated CD19 CAR mRNA targeting CD8 T cells was given in repeated doses to 5 severe SLE patients — all generated CAR in vivo, achieved B-cell depletion, without high-grade CRS (in vivo CAR-T)
- Gamma-delta (γδ) T cells, CAR-NK, CAR-Treg
- Lower risks of severe CRS, ICANS, and GvHD
- CAR-Treg are particularly interesting — aim to enforce antigen-specific tolerance rather than just depleting B cells
- Allogeneic, gene-edited CAR products
- Healthy-donor-derived → standardised, off-the-shelf, rapid availability
- Finite persistence may reduce long-term risks while still delivering intense, time-limited B-lineage depletion
- Bispecific T Cell Engagers (TCEs)
- CD3 × B-cell antigen antibodies
- Blinatumomab (CD19 × CD3) in small RA cohorts: profound B-cell depletion, naïve-skewed reset, rapid clinical/imaging improvement, mostly low-grade infusion reactions
- CD19- and BCMA-directed TCE programmes ongoing in RA, SSc, dermatomyositis, primary Sjögren, and early SLE/LN
7. Mechanism: What “Immune Reset” Actually Means
The authors emphasise that immune reset is more than transient B-cell depletion. Reported features include:
- Deep tissue (not just peripheral blood) B-cell depletion — validated histologically by Tur et al. (ARD 2025)
- Suppression of the type I interferon pathway
- B-cell reconstitution with a predominantly naïve phenotype
- Loss of pathogenic gene-expression signatures
- Durable remission even after B cells return — implying the qualitative nature of the new B-cell pool matters more than absolute count
8. Trial Design and Practical Guidance
The Lupus Clinical Investigators Network (LCIN) consensus document (Caricchio et al., ACR Open Rheumatol 2025) provides discipline-specific guidance covering:
- Patient selection criteria
- Timing and conditions of leukapheresis
- Management of background immunosuppression and glucocorticoids during washout
- CRS and ICANS grading
- Infection prophylaxis
- Long-term follow-up frameworks
The authors flag a paradoxical risk: too many parallel trials are diluting candidate patient pools and resources — calling for smarter trial designs that match patients to the most appropriate trial based on genetic, phenotypic, and disease characteristics.
Key Takeaways for the Practising Rheumatologist
- CD19-directed CAR-T (especially CD19–4-1BB) is currently the most established platform, with consistent signals of deep, drug-free remission in refractory SLE (~80–85% complete response in early-phase trials), and promising responses in IIM and SSc.
- CD19 > CD20 mechanistically because it captures plasmablasts and tissue-resident B cells that anti-CD20 antibodies miss. This explains why even obinutuzumab, despite better depletion than rituximab, cannot fully replace the cellular approach.
- Toxicity in autoimmune disease is qualitatively different from oncology — mostly low-grade CRS, rare ICANS, and a new entity — LICATS — which is organ-specific, self-limited, and must not be confused with disease flare.
- LICATS should not trigger reflexive immunosuppression — recognise it, capture it systematically in trials, treat symptomatically.
- The Fra2 SSc model showing disease exacerbation with B-cell depletion is a sobering reminder that the SLE paradigm may not translate uniformly across autoimmune diseases — IIM patients may also flare via CD8+ expansion. Mechanism matters.
- Brief pulse steroids during washout can safely bridge severe flares without compromising CAR-T efficacy.
- Long-term safety remains uncertain — hypogammaglobulinaemia, infection risk, and the haematology-derived class-wide warning for secondary T-cell malignancies mandate disciplined long-term surveillance.
- The platform landscape is rapidly diversifying — allogeneic CARs, γδ-CARs, CAR-NK, CAR-Tregs, RNA CARs, in-vivo LNP-mRNA CARs, and bispecific T-cell engagers (CD19/CD3, BCMA/CD3) — each with potential trade-offs in persistence, manufacturing burden, and toxicity.
- Access and equity are the looming ethical challenges — cost, infrastructure, leukapheresis capacity, and specialised post-infusion monitoring are not trivial, and the field must plan for this proactively.
- CAR-T is not yet ready as routine therapy — it remains a highly selected, refractory-disease option requiring experienced centres, structured trials, and long-term registries.
Final Take-Home Message
Cellular therapy — particularly CD19-directed CAR-T — represents the first credible attempt at a true immunological reset in autoimmune rheumatic disease, replacing the chronic-suppression paradigm with a one-and-done intervention aimed at qualitatively rebuilding the B-cell compartment. The early efficacy signals in refractory SLE, IIM, and SSc are extraordinary; the toxicity profile in autoimmune cohorts is so far more favourable than in oncology; and the platform diversity (allogeneic, RNA, TCE, NK) suggests this is the beginning, not the endpoint.
For rheumatologists, the responsibilities going forward are clear: rigorous patient selection, long-term surveillance, systematic capture of new toxicities like LICATS, avoidance of duplicative trial competition, and advocacy for equitable access — so that the most transformative therapy our field has seen in a generation does not become available to only a privileged few.