TL;DR: Biologic failure in obesity is not only an inflammation problem but a pharmacokinetic one — weight-driven clearance systematically underdoses patients on fixed-dose subcutaneous biologics, so the dosing strategy (fixed vs weight-based vs banded) should be matched to how strongly weight drives clearance.
The Clinical Problem
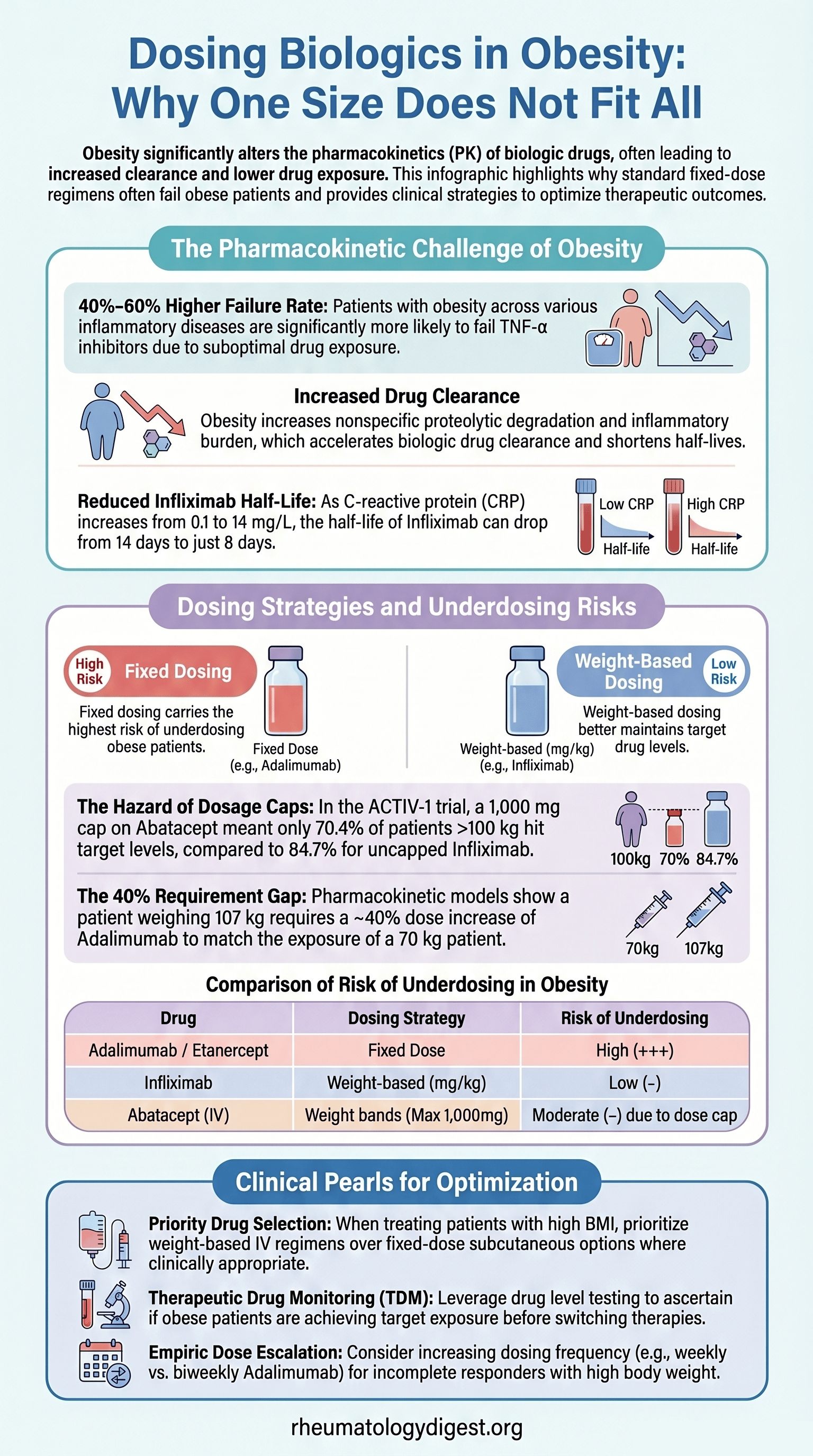
About 1 in 3 patients with RA, PsA and other rheumatic diseases still have active disease after 6–12 months of biologic therapy. Treatment failure is disproportionately common in obesity — patients with obesity are roughly 40–60% more likely to fail TNF-α inhibitors, with reduced responses across other biologic classes too. This is usually blamed on higher pain, worse function and greater inflammatory burden. The authors argue a neglected contributor is pharmacokinetics (PK): many patients with obesity may simply be underdosed, because FDA-labelled regimens were optimised for an “average” patient and early-phase trials frequently excluded or under-sampled people with extreme body sizes.
Why Weight Changes Biologic Exposure
- Rising body weight increases both the volume of distribution and, more importantly, clearance — higher clearance means lower drug levels.
- The mechanism is multifactorial: increased non-specific proteolytic degradation of antibody, plus smaller contributions from inflammatory burden reducing FcRn salvage and increased target-mediated elimination.
- Inflammation itself raises clearance independently. A vivid example: infliximab half-life falls from 14 to 8 days as CRP rises from 0.1 to 14 mg/L. Higher inflammation → faster clearance → lower levels → need for higher dosing.
The Core Concept — Match Dosing Strategy to the Allometric Exponent
Biologics are dosed three ways: fixed, weight-based (mg/kg), or weight bands. The “right” choice depends on how strongly weight drives clearance, captured by the allometric exponent on weight:
- Exponent near 0 → weight barely affects clearance → fixed dosing is appropriate.
- Exponent near 1 → clearance scales with weight → weight-based dosing is appropriate.
The mismatch matrix (the key teaching point):
- Fixed dosing when weight DOES affect clearance → underdoses the heavy, overdoses the light.
- Weight-based dosing when weight does NOT affect clearance → underdoses the light, overdoses the heavy.
Because most rheumatology biologics with meaningful weight-clearance relationships are nonetheless given at fixed SC doses, patients with obesity are systematically at risk of underdosing.
Drug-by-Drug Risk
High underdosing risk in obesity (+++), all fixed SC dosing:
- Adalimumab — exponent ~0.75–0.81
- Etanercept — exponent ~0.67
- Certolizumab — BSA-driven
- Golimumab SC (+++); golimumab IV (mg/kg) is low-risk
- Secukinumab SC (+++); secukinumab IV (mg/kg) is low-risk
Lower / mitigated risk:
- Infliximab (mg/kg) — weight-based, low underdosing risk
- Tocilizumab — IV mg/kg (max 800 mg), SC stratified by <100 / ≥100 kg
- Abatacept — IV weight bands (max 1,000 mg); SC levels are lower in obesity but stay therapeutic
- Ustekinumab — SC stratified by <100 / ≥100 kg
Subtle point: a dosing cap can recreate the underdosing problem even in a weight-based drug — once you hit the ceiling, heavy patients revert to effectively fixed dosing.
The ACTIV-1 Illustration (Severe COVID-19)
A natural experiment, since obesity predisposes to severe COVID-19, the trial was 53–58% obese.
- Single-dose abatacept 10 mg/kg IV (capped at 1,000 mg) vs infliximab 5 mg/kg IV (no cap).
- Higher BMI → progressively lower exposure for both, despite weight-based dosing.
- The cap mattered: among patients >100 kg, only 70.4% reached target levels with capped abatacept vs 84.7% with uncapped infliximab.
- Critical illness independently raised clearance — a reminder that PK is population-specific.
How to Optimise Dosing
Population PK models are the ideal but are underused in rheumatology. Worked examples:
- Adalimumab: a 107 kg patient needs ~40% more drug than a 70 kg patient → pragmatically, move from every-2-weeks to weekly.
- Tocilizumab: a 140 kg patient needs ~43% more to match 70 kg exposure.
In the absence of a popPK model, three practical levers:
- Choose a weight-based agent (e.g. infliximab over adalimumab) — downside: usually requires IV infusion.
- Therapeutic drug monitoring (TDM) — confirm target exposure.
- Empirically up-titrate in incomplete responders — most biologics have a wide safety window, though infection-risk data at higher exposures are conflicting.
Key Takeaways
- Obesity is a PK problem, not just an inflammation problem. Weight-driven clearance can leave obese patients under-exposed, and label dosing rarely accounts for it.
- Match the dosing strategy to the weight–clearance relationship. Fixed dosing suits exponents near 0; weight-based dosing suits exponents near 1. Mismatches (and dose caps) predictably under- or over-dose the extremes.
- Highest-risk practical scenario: fixed-dose subcutaneous TNF inhibitors (adalimumab, etanercept, certolizumab, golimumab-SC) and secukinumab-SC in the patient with obesity who is an incomplete responder.
- Not every obese patient needs more drug. Where labelled dosing is deliberately supratherapeutic, obesity is buffered — e.g. abatacept levels are lower in obesity but >90% still exceed the proposed ~10 µg/mL trough target. Whether adjustment is needed depends on the therapeutic window and exposure–response curve, which is exactly what TDM clarifies.
- Dosing alone won’t fix it. Obesity-related non-response is multifactorial — altered PK, higher inflammatory burden, non-inflammatory pain, and assessment bias (difficulty distinguishing active synovitis from soft-tissue swelling). Optimal dosing should sit alongside weight management and exercise.
- The field’s gap: real-world PK/PD studies in obesity (and other special populations, including children) are urgently needed. Higher-dose strategies raise drug and administration costs, but these must be weighed against the cost of persistently active disease.