TL;DR: The defining 2025 change is that monoclonal TNF-alpha inhibitors — especially infliximab — move to first-line for both induction and maintenance in eye, vascular and parenchymal-CNS Behçet’s, displacing cyclophosphamide (arterial) and the azathioprine-first strategy (CNS), while targets broaden from clinical control to angiographic (eye) and endoscopic (GI) remission.
The Clinical Problem
Behçet’s syndrome (BS) is a variable-vessel vasculitis — it can inflame arteries and veins of any calibre — and this is precisely what makes it so hard to manage with a single algorithm. Several features frame the update:
- Profound heterogeneity. A single label spans uveitis, arterial aneurysms, venous and cerebral sinus thrombosis, intracardiac (right-heart) thrombus, gastrointestinal ulcers, parenchymal CNS lesions, and mucocutaneous/joint disease — each with its own prognosis, treatment response and monitoring needs.
- A relapsing-remitting course that burns out over time. Skin, mucosa and joints relapse frequently; major-organ relapses are sparser but damaging — so therapy must both suppress the current attack and prevent the next, while aiming for eventual tapering.
- Prognosis is not uniform. Male sex, young age at onset, and early disease years predict a more severe, organ-dominant course.
- A shifting drug landscape. Interferon-alpha — historically valuable for eye, mucocutaneous and joint disease — is no longer reliably available in Europe and much of the world. Meanwhile head-to-head bDMARD trials and csDMARD-vs-bDMARD RCTs have appeared since 2018.
- Mimickers can be fatal if missed. Syphilitic uveitis, lymphoma, CNS/GI tuberculosis (especially under TNFαi), and monogenic mimics (A20 haploinsufficiency, trisomy 8–associated autoinflammatory disease) must be excluded before immunosuppressing.
What the Paper Does — Methods Snapshot
- A multidisciplinary task force of 29 members from 11 countries: 19 rheumatologists, 2 ophthalmologists, 1 dermatologist, 1 gastroenterologist, 1 neurologist, 1 health professional, 2 patient research partners, 2 EMEUNET members. 55% (16) were new to the group.
- Research questions generated by Delphi survey, framed as PICOs.
- Two SLRs (registered, PROSPERO CRD42025637593) — one on major-organ involvement, one on mucocutaneous/joint — covering October 2015 to November 2024, using PRISMA, Cochrane RoB for RCTs and Newcastle-Ottawa for observational studies.
- Evidence yield: 7128 articles screened → 83 full-text → 81 studies (9 RCTs, 34 comparative observational, 38 non-comparative observational). Domain coverage: eye 24, vascular 22, GI 14, mucocutaneous 13, nervous system 7, joint 6, leg ulcers 2.
- Voting: ≥75% to change/create a recommendation (then ≥67%, then ≥50% in later rounds). LoA scored 0–10; members also rated feasibility and impact on quality of care, which were used to select 2 quality indicators (joint and arterial domains).
- A subtle methodological point: the switch from the 2009 to the 2011 OCEBM levels of evidence lowered the LoE of several recommendations even though their content was unchanged — so a lower LoE here does not mean weaker clinical conviction.
Headline result: 5 overarching principles + 12 recommendations, organised by organ. Of the 12: 1 new, 7 modified, 4 reworded — none identical to 2018.
The Five Overarching Principles
- A. BS is relapsing-remitting, may be organ/life-threatening, and tends to ameliorate over time. (LoA 9.7 ± 0.8)
- B. The goal is to prevent irreversible organ damage and maximise HRQoL. (9.8 ± 0.5)
- C. Evaluate organ involvement throughout the course and rule out mimickers with appropriate modalities. (9.7 ± 0.8)
- D. Individualise by age, sex, type/severity of involvement, disease duration and patient preference. (9.8 ± 0.4)
- E. A multidisciplinary approach, patient education, shared decision-making, adherence and lifestyle change are essential. (9.8 ± 0.4)
The 12 Recommendations, by Organ
Mucocutaneous involvement
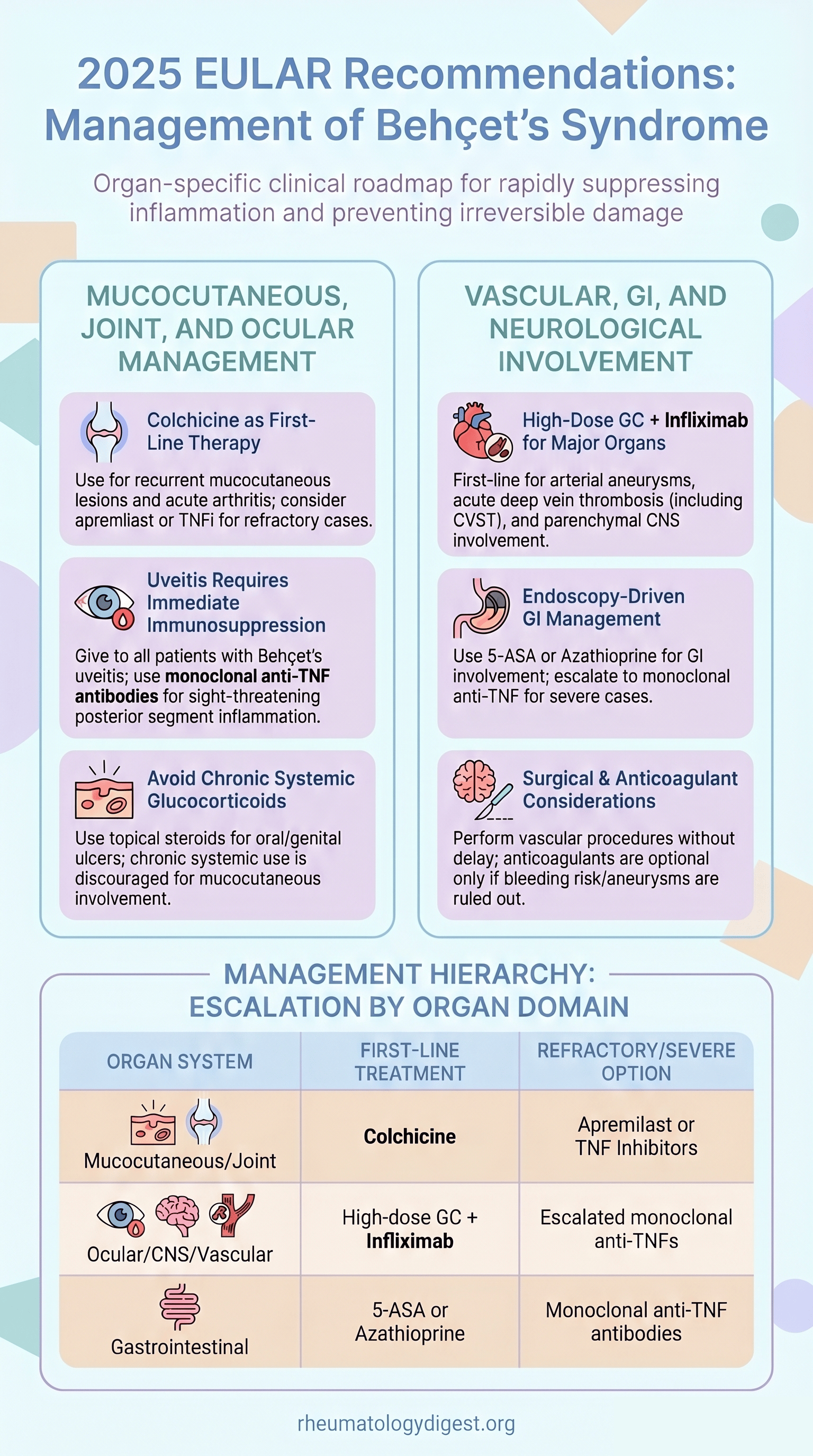
- Colchicine first-line for recurrent mucocutaneous lesions; if refractory/intolerant → apremilast or TNFαi. (LoE 2 / 9.5 ± 0.8)
- Topical measures (e.g. topical GCs) for oral/genital ulcers; avoid chronic systemic glucocorticoids. (LoE 2 topical / 5 systemic GC; 9.0 ± 1.2)
Joint involvement
- Colchicine first-line for acute arthritis; immunosuppressives in recurrent/chronic cases. (LoE 2 / 3; 9.4 ± 1.0)
Eye involvement
- Immunosuppressive therapy in all patients with Behçet’s uveitis, targeting clinical and angiographic remission; monoclonal anti-TNFα (preferably infliximab) + another immunosuppressive for sight-threatening posterior-segment disease; glucocorticoids never as monotherapy. (LoE 2 / 9.7 ± 0.7)
Arterial involvement
- Pulmonary/peripheral artery aneurysms: high-dose GCs + infliximab (cyclophosphamide an alternative); slow GC taper; maintenance with immunosuppressives, preferably monoclonal anti-TNFα. (LoE 2 / 9.8 ± 0.6)
- Don’t delay vascular procedures once medical treatment has started; for pulmonary artery aneurysms at high bleeding risk, embolisation over open surgery. (LoE 4 / 5; 9.7 ± 0.5)
Venous involvement
- Acute deep-vein thrombosis (including cerebral venous sinuses): GCs + immunosuppressives, preferably monoclonal anti-TNFα, continued as maintenance. (LoE 2 / 3; 9.7 ± 0.7)
- Anticoagulants may be added only if bleeding risk is low and pulmonary artery aneurysms are excluded. (LoE 5 / 8.7 ± 1.2 — the lowest LoA in the set)
- In CVST with vision-threatening intracranial hypertension, consider surgical intervention promptly. (LoE 5 / 9.0 ± 1.5)
Gastrointestinal involvement
- Diagnosis, severity assessment and management based on endoscopy. (LoE 5 / 9.5 ± 0.9)
- 5-ASA or azathioprine ± GCs; severe/refractory → monoclonal anti-TNFα. (LoE 3 / 9.6 ± 0.7)
Parenchymal nervous system involvement
- Active parenchymal disease: high-dose GCs + immunosuppressives, preferably infliximab; slow GC taper; immunosuppressive maintenance. (LoE 2 / 9.8 ± 0.4)
Key Takeaways and Not-So-Obvious Details
1. The central shift: earlier, first-line monoclonal TNFαi for major-organ disease. For eye, vascular and nervous system involvement, monoclonal anti-TNFα antibodies are now preferred for both induction and maintenance — not just for csDMARD-refractory patients as in 2018. The rationale is the imperative to suppress inflammation rapidly to prevent irreversible damage, backed by data showing superiority over csDMARDs. Wider biosimilar availability makes this feasible economically (though there are no comparative biosimilar studies in BS).
2. Arterial involvement — infliximab dethrones cyclophosphamide. A major change: high-dose GCs + infliximab is now first-line for pulmonary/peripheral artery aneurysms, with CYC relegated to alternative status. The pivotal new evidence is the Saadoun RCT (NEJM Evidence) — infliximab vs CYC in vascular/NS disease (only 19 vs 18 vascular patients) — showing higher remission at week 24 and fewer mild/moderate adverse events with infliximab (severe AEs similar). Maintenance also shifts from azathioprine to monoclonal TNFαi; the task force suggests continuing ≥5 years. (Typical induction: IV methylprednisolone 1 g × 3 days, then ~1 mg/kg/d oral, tapered over 6–12 months.)
3. Interferon-alpha — written out, but not forgotten. Because of severe supply shortages (including pegylated forms), IFN-α was removed from the recommendation wording yet retained in the text as an effective option for eye, mucocutaneous, joint and venous disease. The task force explicitly states many patients would benefit if its manufacture restarted.
4. Refractory mucocutaneous disease — apremilast or TNFαi, now formally positioned. Apremilast has 2 supportive RCTs (oral/genital ulcers, QoL, good safety). A small head-to-head RCT (adalimumab vs infliximab) showed 6-month mucocutaneous remission of 100% (ADA) vs 86% (IFX), with a notably faster median time to response with adalimumab (42 vs 152 days, P = .002). Thalidomide and dapsone are no longer preferred (adverse-event burden) — reserved as last resorts in resource-limited settings under experienced specialists.
5. Uveitis — richer nuance than the headline suggests.
- GCs never as monotherapy; start 0.5–1 mg/kg/d. Infliximab outperformed IV methylprednisolone pulses in earlier work.
- The Zhong head-to-head RCT (adalimumab vs IFN-α vs ciclosporin-A) found adalimumab superior to ciclosporin with lower annual relapse, and comparable to IFN-α — though criticised for limited external validity (long prior inadequate treatment, prolonged prednisone).
- No RCT compares two TNFαi in uveitis, but consensus holds IV infliximab acts faster while adalimumab has better long-term drug survival/compliance.
- In relapse on a monoclonal TNFαi, escalate the current agent (shorten interval / raise dose) before switching.
- Angiographic remission is now part of the target — FFA leakage predicts long-term relapse, so FFA is advised at least when treatment changes (including tapering) are planned.
- Young men with anterior uveitis warrant azathioprine (high risk of posterior progression); vitreous cells at baseline flag that risk; hypopyon uveitis always needs immunosuppression (it signals retinal vasculitis).
- No reliable withdrawal data — bDMARDs should be continued long term.
6. Venous disease — and the anticoagulation caveat that matters most. First-line TNFαi may be preferred given serious potential morbidity (post-thrombotic syndrome, Budd-Chiari, intracranial hypertension/blindness). Observational data: 45% relapsed on azathioprine, with IFN-α and adalimumab outperforming csDMARDs. Critically — anticoagulation has no controlled evidence, and adding it did not improve outcomes in the available study. The task force does not recommend against it but urges caution: arterial aneurysms accompany or precede venous thrombosis in most patients and can be fatal with anticoagulation — hence exclude pulmonary artery aneurysms first. Optimal duration is unknown.
7. Gastrointestinal disease — endoscopy is non-negotiable. Endoscopy drives diagnosis, mimicker exclusion (Crohn’s, UC, NSAID ulcers, TB), severity grading and monitoring. High-risk ulcer morphology — volcano-type, deep, or >2 cm — prompts TNFαi due to bleeding/perforation risk. Infliximab is preferred for its rapid attainment of high serum concentrations. A practical warning: high-dose GCs may mask perforation. JAKi case series are promising but high-RoB.
8. Parenchymal CNS — TNFαi moves first-line, ciclosporin moves out. Severe flares: IV MP 1 g pulses, repeatable up to 7–10 times in poor responders, then 1 mg/kg/d oral. The old azathioprine-first/TNFαi-rescue approach is reversed — infliximab is now first-line (high disability risk; allows faster GC taper). Maintenance ≥5 years, especially in younger patients. Importantly, ciclosporin-A should be avoided in nervous-system involvement (meta-analysis links it to increased NS disease) — formerly a standalone 2018 recommendation, now demoted to text given declining CsA use. Tocilizumab is only weakly supported (uncontrolled, high-RoB) and can paradoxically trigger mucocutaneous flares.
9. Geography shapes the disease — and the guidance. GI involvement clusters in the Far East, vascular disease in the Middle East, and the pathergy reaction is rare in Europe. The 11-country task force deliberately built options for differing drug availability, reimbursement and background risks (e.g. latent TB before TNFαi).
10. Honest limitations. Trial-population and outcome heterogeneity precluded any meta-analysis or cross-drug comparison; RCTs were small; sex-disaggregated data were largely missing despite known sex differences in severity; and patient-important outcomes (fatigue, work disability) were absent from drug trials. A BS core outcome set is still in development.
Final Take-Aways
- One disease, many algorithms: management is organ-specific by design — aggressive upfront for organ/life-threatening disease, step-up (colchicine-led) for mucocutaneous/joint disease guided by patient preference.
- The defining 2025 change: monoclonal TNFαi (especially infliximab) move to first-line for eye, vascular and parenchymal-CNS disease, for both induction and maintenance — displacing cyclophosphamide (arterial) and the azathioprine-first strategy (CNS).
- Targets are broadening: beyond clinical control to angiographic remission (eye) and endoscopic remission (GI), reflecting damage-prevention as the overarching goal.
- Use caution with the soft spots: anticoagulation only after excluding pulmonary aneurysms; ciclosporin avoided in CNS disease; chronic systemic steroids avoided in skin-only disease.
- The evidence base is still thin: small, heterogeneous RCTs, no meta-analysis possible, and big gaps in monitoring strategy, tapering/withdrawal, pregnancy, biosimilars, and patient-reported outcomes — all populating a detailed research agenda.