TL;DR: The 2025 EULAR update is the most streamlined yet — 5 principles and 9 recommendations, all with unusually high consensus — and its single biggest shift is abandoning post-methotrexate prognostic stratification: because MTX + glucocorticoid failure is itself a poor-prognosis signal, advance straight to a b/tsDMARD rather than detouring through a second csDMARD.
The Clinical Problem
RA management is fundamentally a problem of sequencing and balancing — choosing among an ever-growing arsenal of csDMARDs, bDMARDs and tsDMARDs (JAKi) while weighing efficacy, safety and cost across very different health systems. Several realities frame this update:
- Efficacy has plateaued at the group level. Across mechanisms, licensed targeted DMARDs show broadly similar group-level efficacy. The major unmet need is predicting who responds to what — and no validated individual-level predictor exists.
- Cure remains rare. Even in sustained remission, stopping DMARDs is followed by flares in the vast majority of patients.
- A refractory tail persists. Roughly 20–30% of patients in affluent countries (and many more elsewhere) never reach target, giving rise to the formal concept of difficult-to-treat (D2T) RA.
- No new drug class has been approved in Europe or the USA in ~6 years — so this update is about strategy refinement, not new agents.
- Pre-RA prevention has failed so far — interventions delay but do not prevent classifiable RA.
What the Paper Does — Methods Snapshot
- An International Task Force of 50 members (the largest ever assembled for this purpose) — rheumatologists across Europe, Asia, Latin America, North America, Africa and Australia, plus an infectious disease specialist, patient research partners (3) and non-medical health professionals (3).
- Steering committee of 15 met in Washington DC (Nov 2024); full task force convened in Amsterdam (Mar 2025).
- Two systematic literature reviews (SLRs) — one on efficacy, one on safety — covering evidence published from early 2022 up to end of January 2025.
- OCEBM used for Levels of Evidence (LoE) and Grades of Recommendation (GoR); AGREE II framework followed.
- Voting thresholds: changing or approving wording required >75% for immediate acceptance; failing that, a second round needed >67%, then a third needed >50%; below that the item was rejected.
- Level of Agreement (LoA): anonymous post-meeting vote, 0–10 scale, reported as mean ± SD.
The task force trimmed to 5 overarching principles + 9 recommendations (down from 11 in 2022 — the smallest set in this guideline’s history). For the first time every single item scored a mean LoA above 9/10, signalling unusually high consensus maturity.
The Five Overarching Principles
All retained, with only minor wordsmithing:
- A. Care is aimed at best care, based on shared decision-making. (LoA 9.98 ± 0.14)
- B. Decisions rest on disease activity, safety and patient factors (comorbidities, structural damage). (LoA 9.88 ± 0.44)
- C. Rheumatologists are the primary specialists for RA. (LoA 9.72 ± 0.57 — 61% wanted to reword this, but it fell short of the 75% threshold and was kept.)
- D. Patients need access to multiple modes of action and may need successive therapies for life. (LoA 9.94 ± 0.24)
- E. RA carries high individual, medical and societal costs to be factored in. (LoA 9.58 ± 0.73)
The Nine Recommendations
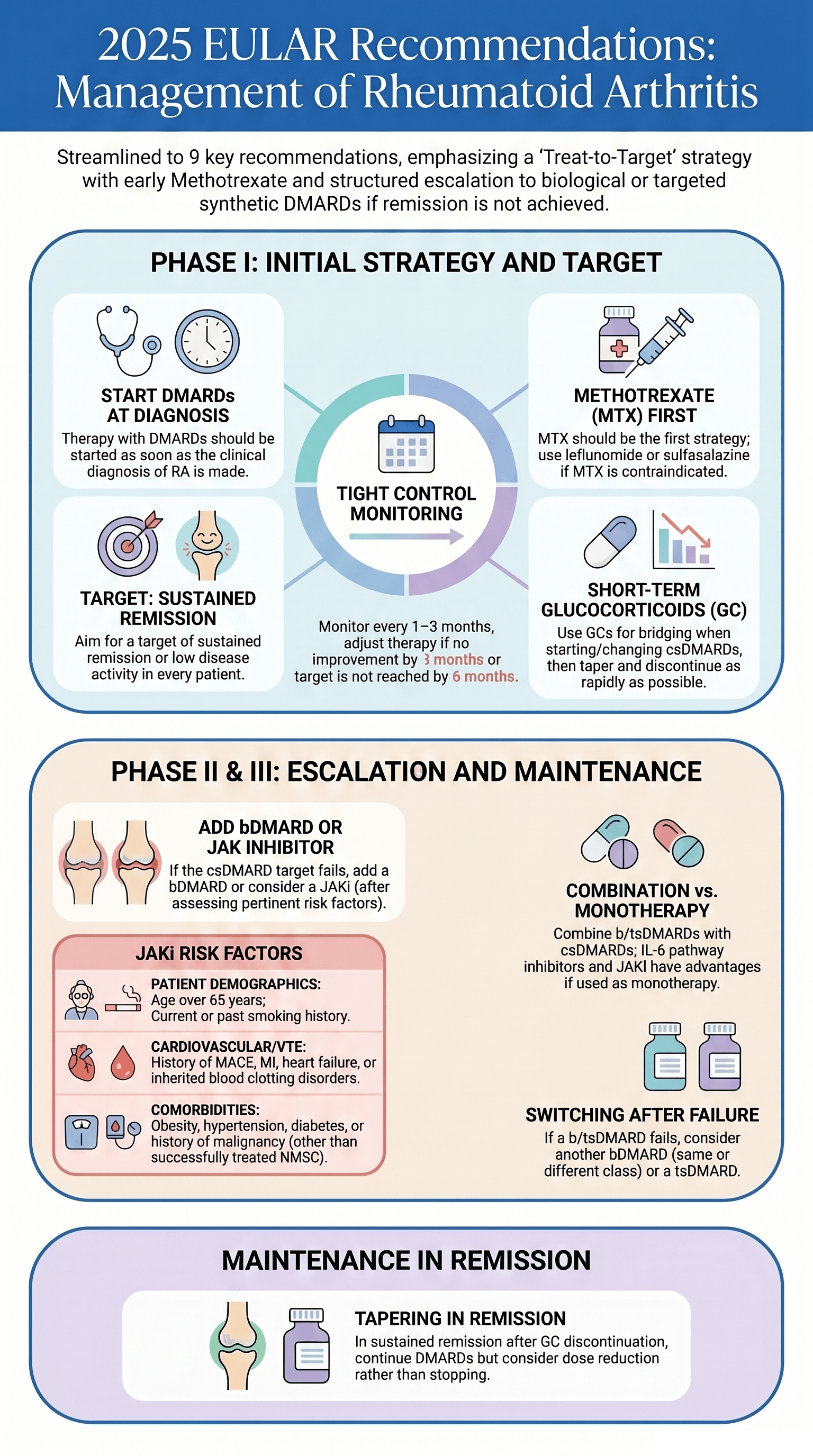
- Start DMARDs as soon as RA is diagnosed. (1a / A / 9.92) — diagnosis is clinical; the defining feature is clinical joint swelling (synovitis). Classification criteria support but do not replace diagnosis; US/MRI are explicitly not diagnostic.
- Treat-to-target: sustained remission or low disease activity (LDA) in every patient. (1a / A / 9.82) — remission is the goal especially in early RA; LDA is acceptable in long-standing/multi-failure disease. T2T means ≥50% disease-activity reduction by 3 months and target attainment by 6 months.
- Frequent disease-activity monitoring (every 1–3 months) in active disease; adjust therapy if no improvement by 3 months or target unmet by 6 months; reduce frequency once sustained. (LoA 9.62)
- MTX is part of the first strategy; if contraindicated or early-intolerant, use leflunomide or sulfasalazine. (1a / A / 9.38) — old recs 4 and 5 merged here.
- Short-term glucocorticoids when starting/changing csDMARDs, tapered and stopped as fast as clinically feasible. (1a / A / 9.46) — kept by 98%, the largest majority ever recorded for GC bridging.
- If csDMARD strategy fails → add a bDMARD; JAKi may be considered, but pertinent risk factors must be weighed. (Efficacy 1a/A; Safety 2a/B; LoA 9.28) — the single biggest change in this update.
- Combine b/tsDMARDs with a csDMARD; where csDMARD comedication isn’t possible, IL-6 pathway inhibitors and JAKi may have advantages over other bDMARDs as monotherapy. (1a / A / 9.48)
- After b/tsDMARD failure → switch to another b/tsDMARD; after a single TNF or IL-6R inhibitor failure, either change mechanism or try a second TNF/IL-6R inhibitor. (LoA 9.48) — kept by 100%. A drug of the same class should not be used a third time.
- After GCs are stopped and remission is sustained, continue DMARDs; dose reduction (or interval lengthening) may be considered. (1b / A / 9.56)
Key Takeaways and Not-So-Obvious Details
1. The end of prognostic-risk stratification (the headline change). Old recommendations 7 and 8 stratified post-MTX patients by poor-prognosis markers (high SJC/APR, autoantibodies, early erosions, ≥2 csDMARD failures) — biologics/JAKi for “high-risk,” another csDMARD for “low-risk.” This stratification is abandoned (98% vote to delete). The low-risk arm rested mainly on expert opinion; a second csDMARD shows much lower persistence and limited efficacy after MTX failure; and failure of MTX+GC is itself a poor prognostic sign. Falling biosimilar prices and generic tofacitinib removed much of the economic rationale for the csDMARD detour. This does not mean prognostic factors are irrelevant, nor that a second csDMARD is forbidden (still reasonable in resource-limited settings).
2. No first-line biologics. Despite cheaper biosimilars, no trial has shown superiority of bDMARDs over MTX + GC in early RA clinically, functionally or radiographically. The “should” in rec 4 was deliberately not softened to “could,” to avoid implying biologics-first.
3. Triple therapy stays out. Recent NORD-STAR data reinforce this: triple therapy (MTX/SSZ/HCQ) + intra-articular GC offered no advantage over MTX + oral GC at 6 months — and showed more radiographic progression (27% vs 5% in the MTX+GC arm).
4. DAS28 is discouraged for defining remission. It over-weights tender joints and acute-phase reactants. IL-6–targeting agents and JAKi blunt CRP/ESR independently of clinical improvement, inflating DAS28 remission rates while patients still have active disease. Use ACR-EULAR Boolean or index-based (CDAI/SDAI) definitions. (The 2022 Boolean revision now permits PGA up to 2 cm, vs 1 cm previously.)
5. Imaging remission is not a target. US-guided (TaSER, ARCTIC) and MRI-guided (IMAGINE-RA) remission strategies are not superior to clinical remission and add adverse events and cost.
6. A more lenient lab-monitoring stance. The dedicated SLR on DMARD monitoring found no eligible studies — yet observational data show lab abnormalities beyond 3–6 months are infrequent and minor, with most adverse events clustering in the first 3–6 months. Once a drug is tolerated for ~3–6 months, lab monitoring may drop to semiannual or less (demonstrated for csDMARDs, now extended to bDMARDs). Caveat: infections cannot be “monitored,” and individual comorbidities may demand more.
7. JAKi positioning is unchanged — and deliberately so. Proposals ranged from deleting the safety caveat (most observational data have not confirmed ORAL Surveillance concerns) to restricting JAKi to post-bDMARD use. Neither passed; 81% kept the wording. JAKi sit at the same level as bDMARDs, contingent on risk assessment. The relevant risk factors: age >65, current/past smoking, CV and malignancy risk, and VTE risk (prior MI/HF, inherited clotting disorders, prior clots, combined hormonal contraceptives/HRT, major surgery, immobility). A post-hoc ORAL Surveillance analysis suggests statins may mitigate tofacitinib CV risk — hypothesis-generating only.
8. Therapeutic drug monitoring (TDM) is not recommended. The ADDORA-switch trial showed TDM does not improve outcomes versus routine care, and it does not aid response prediction — so it isn’t worth the cost.
9. Cycling within the JAKi class is acceptable. No RCT exists, but positive observational data (JAK-pot) support it — though never a third drug of the same class.
10. Tapering, not stopping. Position strengthened: dose-reduce or lengthen intervals after ≥6 months of sustained remission, but do not stop — withdrawal triggers flares in most patients within a year.
11. Pre-RA is intentionally excluded. Prevention trials (PRAIRI/rituximab, ARIAA & ALTO/abatacept) delayed but did not prevent RA; only DINORA (anti-TNF+MTX in very early arthritis) hinted at durable remission, unconfirmed. These recommendations apply only to diagnosed RA.
12. RA-ILD: acknowledged but not actionable yet. Nintedanib (INBUILD subanalysis) and pirfenidone (phase 2) slow lung-function decline, but they are antifibrotics, not RA DMARDs — evidence was deemed insufficient for a dedicated item. Involve a pulmonologist.
13. Predicting response remains unsolved. R4RA (rituximab vs tocilizumab by synovial B-cell signature) showed no significant difference at primary endpoint. Very high CRP (anti-IL-6R response) and high RF (differential TNFi response) are suggestive but only from post-hoc/observational data.
Final Take-Aways
- Simpler, not weaker: 9 recommendations, all with LoA >9 — the most streamlined and most agreed-upon set yet.
- The algorithm is unchanged in spine: Phase I = MTX + short-term GC (or LEF/SSZ if MTX contraindicated); Phase II = add a bDMARD (JAKi only after risk assessment); Phase III = switch b/tsDMARD — all under a T2T discipline (50%/3 mo, target/6 mo).
- The conceptual shift: MTX+GC failure is itself a poor-prognosis signal — so advance to a b/tsDMARD rather than detouring through another csDMARD (economics permitting).
- Safety is individualised, not drug-class-phobic: JAKi remain co-equal with bDMARDs after honest risk stratification; monitoring can be liberalised after the early high-risk window.
- The persistent gaps: no response predictors, no cure (tapering yes, stopping no), no validated pre-RA prevention, and a 20–30% refractory tail driving the D2T and research agendas.