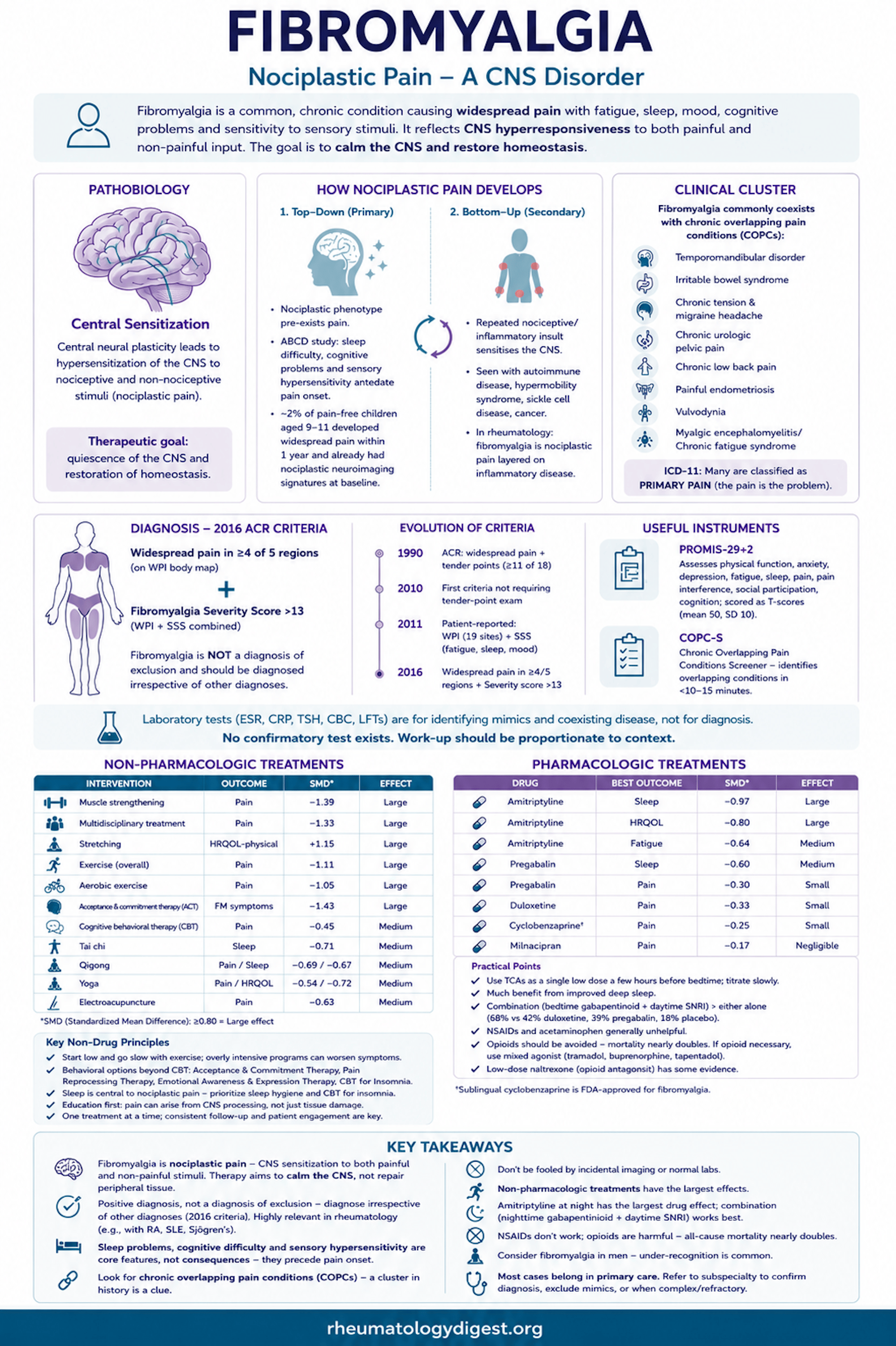
TL;DR: Fibromyalgia is nociplastic pain — CNS sensitisation to both painful and non-painful stimuli — so the goal is to calm a hyperresponsive CNS, not repair peripheral tissue; it is a positive diagnosis made irrespective of other diagnoses (so coexisting fibromyalgia in RA or SLE does not warrant more immunosuppression), non-pharmacologic treatment outperforms drugs, amitriptyline at night is the drug with the largest effect, and opioids are harmful.
The Case That Frames the Article
A 43-year-old man with 3 years of chronic low back pain, already failed on muscle relaxants, NSAIDs, epidural steroid injections, and physical therapy.
- Work-up normal: ESR, CRP, TSH, CBC, LFTs.
- MRI lumbar spine: mild degenerative change and a protruding disc at L5/S1 — a convenient but misleading “answer.”
- Body map: pain in back, head, shoulders, and legs.
- History: tension headache, non-cardiac chest pain, prior diagnosis of chronic prostatitis, long-standing insomnia, fatigue, sensitivity to bright lights, multiple drug allergies.
- Examination: widespread tenderness, but normal strength and sensation; negative provocative manoeuvres of the lower back and sacroiliac joint.
- He is asking whether he should have lumbar surgery or start opioids.
The authors chose a male patient deliberately, because clinicians disproportionately consider fibromyalgia only in women — a diagnostic blind spot with real consequences.
The Clinical Problem
Fibromyalgia affects roughly 4–6% of the US population, with similar prevalence worldwide, and — like most chronic pain conditions — is 1.5 to 2 times more common in women and girls. Healthcare costs have been estimated at around three times those of matched controls.
The cardinal feature is persistent widespread pain, but the syndrome is really a cluster: sleep disturbance, fatigue, mood problems, memory/cognitive difficulty, and sensitivity to non-painful sensory stimuli — lights, noises, odours.
The conceptual history matters for how we talk to patients. The condition was once called fibrositis, on the assumption of inflamed, tender muscle. When no peripheral inflammation could be found, the name shifted to fibromyalgia — and the absence of visible tissue pathology led many clinicians to question whether the condition was real at all. That scepticism still colours consultations today.
Two decades of research have since produced objective neurobiologic underpinnings, supporting the International Association for the Study of Pain’s formal recognition of a third pain mechanism:
Nociplastic pain — pain arising from central neural plasticity and CNS sensitisation, with little or no input from peripheral tissue.
This is the single most important conceptual shift in the article. In fibromyalgia the CNS is hyperresponsive to sensory input in general, both noxious and innocuous. Therefore: the therapeutic goal is not to “fix” a peripheral lesion, but to calm CNS hyperresponsiveness and restore homeostasis.
Chronic Overlapping Pain Conditions (COPCs)
In 2016 the NIH identified 10 chronic pain conditions that cluster with fibromyalgia, affect women more than men, resist conventional biomedical intervention, and are probably nociplastic in mechanism — including temporomandibular disorder, IBS, chronic tension and migraine headache, chronic urologic pelvic pain, chronic low back pain, painful endometriosis, vulvodynia, and myalgic encephalomyelitis/CFS. ICD-11 now classifies many of these as primary pain (the pain is the problem) as opposed to secondary pain (pain due to another disease, e.g. osteoarthritis).
Look back at the vignette: tension headache, non-cardiac chest pain, chronic prostatitis, chronic low back pain. The COPC pattern was in the history all along.
How Nociplastic Pain Develops — Two Routes
- Top-down (CNS-driven, primary): The nociplastic phenotype exists before pain does. In the large ABCD study, sleep difficulty, memory problems, and sensory hypersensitivity — alone or combined — antedated the onset of pain. These are therefore core components, not consequences, of nociplastic pain. In a companion ABCD analysis, pain-free children aged 9–11 underwent baseline brain imaging; roughly 2% developed widespread pain within a year, and those children already showed nociplastic neuroimaging signatures at baseline, before any pain.
- Bottom-up (secondary): Repeated nociceptive or inflammatory insult progressively sensitises the CNS — seen with autoimmune disease, hypermobility syndrome, sickle cell disease, and cancer. This is the mechanism most relevant to rheumatology practice: fibromyalgia superimposed on RA, SLE, or Sjögren’s is nociplastic pain layered on inflammatory disease, and it will not respond to further immunosuppression.
Diagnosis — How the Criteria Evolved
- 1990 ACR: widespread pain + tender points (≥11 of 18).
- 2010: first criteria not requiring tender-point examination.
- 2011: entirely patient-reported, with two components — the Widespread Pain Index (WPI), capturing chronic pain at 19 sites, and the Symptom Severity Score (SSS), capturing fatigue, sleep problems, and depressed mood.
- 2016 revision: widespread pain redefined as pain in ≥4 of 5 regions on the WPI body map, with a Fibromyalgia Severity score >13 (WPI + SSS combined). Critically — fibromyalgia is explicitly NOT a diagnosis of exclusion and should be diagnosed irrespective of other diagnoses.
The Fibromyalgia Severity score is continuous, and can serve as a proxy measure of the degree of nociplasticity — useful for tracking.
Useful instruments:
- PROMIS-29+2 — physical function, anxiety, depression, fatigue, sleep, pain, pain interference, social participation, cognition; scored as T-scores (mean 50, SD 10) against population norms.
- COPC-S (Chronic Overlapping Pain Conditions Screener) — patient-completed, identifies the overlapping conditions in under 10–15 minutes.
Laboratory testing is for identifying mimics and coexisting disease, not for diagnosing fibromyalgia: ESR, CRP, TSH, CBC, LFTs. There is no confirmatory test. Work-up should be proportionate to context: childhood-onset, slowly evolving widespread pain needs very little work-up; acute or subacute onset warrants a more extensive evaluation.
Management
Most fibromyalgia can and should be managed in primary care. Refer to rheumatology/neurology only to confirm the diagnosis, exclude mimics, or when disease is complex or refractory — often a one-time consultation suffices.
Three framing principles the authors stress:
- All available therapies have modest effect sizes at best — several attempts are usually needed to find the right combination.
- Introduce one treatment at a time to judge benefit and side effects.
- Patient engagement is decisive, because most effective interventions are non-pharmacologic and require active participation.
Education and self-care — the foundation. Patients often assume pain must mean tissue damage; explicit reassurance that pain can arise from CNS processing is therapeutic in itself. Core messaging: fibromyalgia is chronic and not curable, but manageable and not life-threatening; treatment targets a hypersensitive CNS; self-care matters. Self-care domains include pain education, sleep hygiene, activity pacing, stress management, social support, graded physical activity, pleasant activity scheduling, resilience training, dietary modification, and environmental/ergonomic adjustment — each requiring habit formation, so consistency and follow-up encouragement matter. (PainGuide — painguide.com — is cited as a patient resource.)
Non-pharmacologic treatments carry the largest effect sizes (SMD, where ≥0.80 = large):
| Intervention | Outcome | SMD | Effect |
|---|---|---|---|
| Muscle strengthening | Pain | −1.39 | Large |
| Multidisciplinary treatment | Pain | −1.33 | Large |
| Stretching | HRQOL-physical | +1.15 | Large |
| Exercise (overall) | Pain | −1.11 | Large |
| Aerobic exercise | Pain | −1.05 | Large |
| Acceptance & commitment therapy | FM symptoms | −1.43 | Large |
| CBT | Pain | −0.45 | Medium |
| Tai chi | Sleep | −0.71 | Medium |
| Qigong | Pain / sleep | −0.69 / −0.67 | Medium |
| Yoga | Pain / HRQOL | −0.54 / −0.72 | Medium |
| Electroacupuncture | Pain | −0.63 | Medium |
Exercise works — but “start low and go slow”, because physical therapy delivered too aggressively can exacerbate symptoms. Behavioural options beyond standard CBT include acceptance and commitment therapy, pain reprocessing therapy (retraining the brain to read harmless sensations as safe), emotional awareness and expression therapy, and CBT for insomnia — the last justified by sleep’s central role in nociplastic pain.
Pharmacologic treatments — smaller effects than the non-drug options:
| Drug | Best outcome | SMD | Effect |
|---|---|---|---|
| Amitriptyline | Sleep | −0.97 | Large |
| Amitriptyline | HRQOL | −0.80 | Large |
| Amitriptyline | Fatigue | −0.64 | Medium |
| Pregabalin | Sleep | −0.60 | Medium |
| Pregabalin | Pain | −0.30 | Small |
| Duloxetine | Pain | −0.33 | Small |
| Cyclobenzaprine | Pain | −0.25 | Small |
| Milnacipran | Pain | −0.17 | Negligible |
Practical points:
- Tricyclics work best as a single low dose a few hours before bedtime, exploiting the hypnotic effect; titrate slowly until sleep improves. Amitriptyline and nortriptyline are the classics; sublingual cyclobenzaprine is now FDA-approved for fibromyalgia.
- Much of the benefit of tricyclics and gabapentinoids appears to come from improved deep sleep.
- SNRIs work independently of any antidepressant effect. Agents with greater noradrenergic activity (duloxetine, milnacipran) outperform highly selective SSRIs; pure noradrenaline-reuptake inhibitors such as esreboxetine are also efficacious.
- Combination beats monotherapy. In one trial, a gabapentinoid at bedtime plus an SNRI during the day achieved moderate-or-greater global pain relief in 68%, versus 42% duloxetine alone, 39% pregabalin alone, and 18% placebo.
- NSAIDs and acetaminophen are generally unhelpful — though they may be appropriate for a genuinely coexisting nociceptive condition such as osteoarthritis.
- Opioids should be avoided. Excess endogenous opioid release may itself promote nociplastic pain via opioid-induced hyperalgesia; overdose and addiction are risks; and all-cause mortality nearly doubles with opioid use (myocardial infarction, falls, suicide, motor vehicle collisions). If an opioid must be used, a mixed agonist (tramadol, buprenorphine, tapentadol) is preferable. Intriguingly, low-dose naltrexone — an opioid antagonist — has some supporting evidence.
Guidelines (Canadian, American Family Physician, EULAR) converge on the same three principles: multidisciplinary rather than single-modality treatment, patient education first, and active patient participation.
Areas of Uncertainty
- No blood test or biomarker has succeeded, partly because the underlying pathophysiology has been misconstrued.
- Claims that fibromyalgia is an autoimmune disorder, a small-fibre neuropathy, or fundamentally a psychological problem remain unsubstantiated. Reduced intraepidermal nerve fibre density does occur, but small-fibre neuropathy is a highly non-specific finding across hundreds of conditions, occurs with or without pain, and has no established pathogenic role here. Similarly, psychiatric comorbidity can result from inadequately treated pain, with little evidence it is the primary cause.
- Emerging: neurostimulation (tDCS, TMS, TENS), cannabinoids (whether CBD alone suffices or some THC is needed remains open), brief behavioural interventions, light-based therapy, low-intensity focused ultrasound to deep brain regions, psychedelics, and resilience training.
Key Takeaways
- Fibromyalgia is nociplastic pain — CNS sensitisation to both painful and non-painful stimuli. Therapy aims to calm the CNS, not repair peripheral tissue.
- It is a positive diagnosis, not a diagnosis of exclusion — and per the 2016 criteria, it should be diagnosed irrespective of other diagnoses. Directly relevant to rheumatology: fibromyalgia coexisting with RA or SLE is common and does not warrant escalating immunosuppression.
- Sleep problems, cognitive difficulty, and sensory hypersensitivity are core features, not consequences — ABCD data show they precede pain onset, and imaging signatures precede pain by a year.
- Look for the chronic overlapping pain conditions. Tension headache, IBS, chronic pelvic pain, TMD, and non-cardiac chest pain in one history should reframe the whole clinical picture.
- Don’t be fooled by incidental imaging. A protruding disc on MRI is not an explanation for widespread pain with negative provocative testing.
- Non-pharmacologic treatment outperforms drugs. Exercise (especially strengthening), multidisciplinary care, ACT, CBT, tai chi, qigong and yoga carry medium-to-large effect sizes; every approved drug is small-to-medium at best.
- “Start low and go slow” with exercise — poorly graded physical therapy makes symptoms worse.
- Amitriptyline at night is the drug with the largest effect size, driven substantially by improved sleep; combination (nighttime gabapentinoid + daytime SNRI) beats either alone.
- NSAIDs don’t work; opioids are harmful — all-cause mortality nearly doubles. Low-dose naltrexone is an interesting counterpoint.
- Consider it in men. The vignette was deliberately male — under-recognition in men is a real diagnostic failure.
- Most cases belong in primary care. Subspecialty referral is for diagnostic confirmation or exclusion of mimics, often as a single consultation.
- The authors’ plan for the vignette patient: reassure that surgery is not indicated, start a low nighttime dose of a tricyclic (cyclobenzaprine or nortriptyline) plus a graduated activity programme (walking or yoga); if inadequate, move to other centrally acting non-opioid agents (SNRIs, gabapentinoids) and integrative therapies including CBT, movement therapy, and neurostimulation.