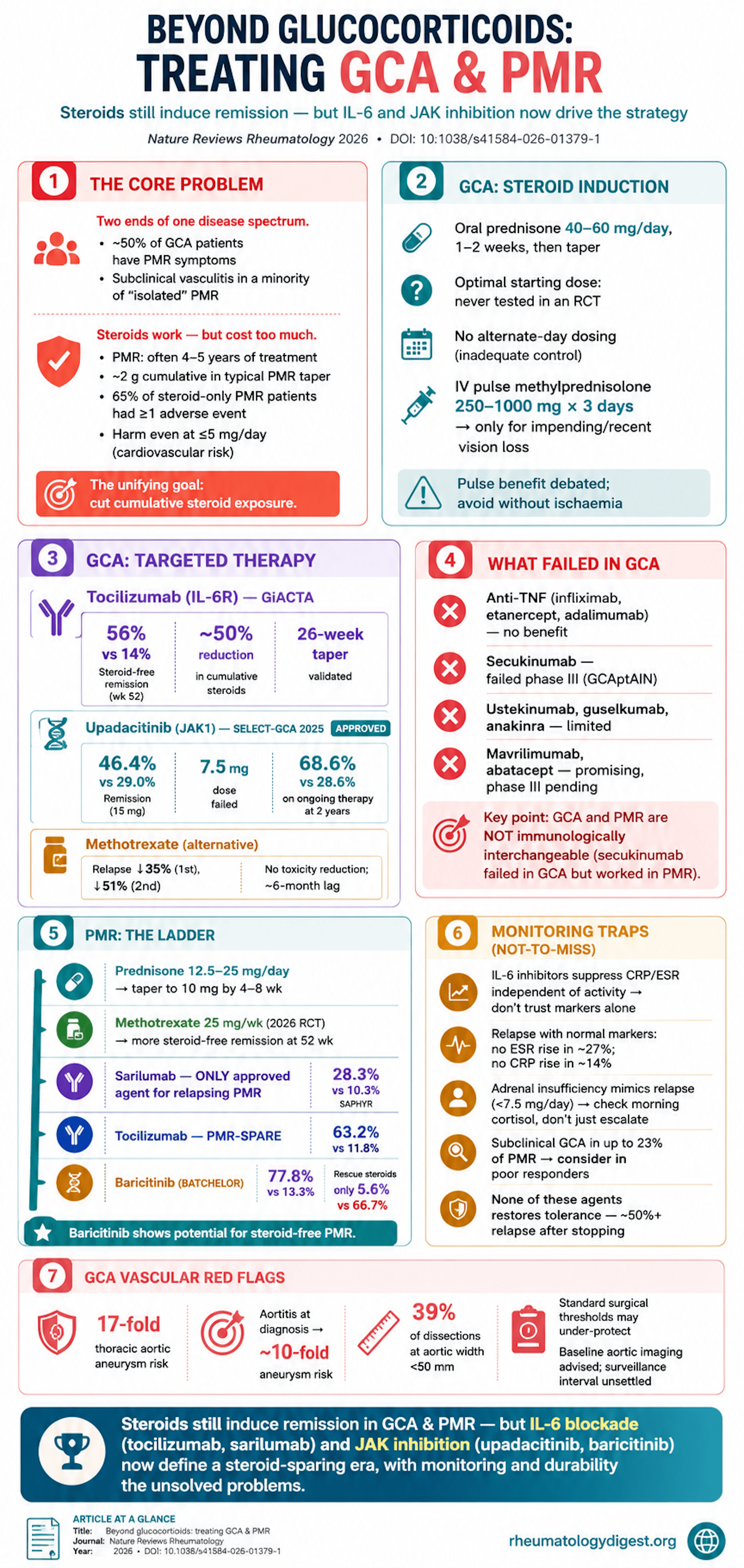
TL;DR: Glucocorticoids still induce remission in GCA and PMR but their cumulative toxicity has driven a decisive pivot to steroid-sparing therapy — IL-6 receptor inhibition (tocilizumab in GCA, sarilumab in PMR) and now JAK inhibition (upadacitinib approved for GCA) roughly halve cumulative steroids and cut relapse, yet none reliably delivers durable treatment-free remission, and monitoring remains a genuine weak point.
The Clinical Problem
Giant cell arteritis (GCA) and polymyalgia rheumatica (PMR) are among the commonest inflammatory rheumatic diseases of older adults, and although historically treated as separate entities, they are increasingly understood as two ends of a shared disease continuum. Roughly half of GCA patients have PMR symptoms, and subclinical large-vessel vasculitis is detectable in a meaningful minority of apparently isolated PMR.
For both conditions, glucocorticoids remain the cornerstone — they rapidly suppress inflammation and, in GCA specifically, reduce the risk of ischaemic vision loss. But that cornerstone is also the problem:
- Therapy is typically prolonged — many PMR patients remain on steroids 4–5 years, and a substantial fraction of both diseases relapse during tapering.
- Cumulative glucocorticoid exposure drives serious morbidity: osteoporosis, fractures, diabetes, hypertension, infection, cataract, frailty, and cardiovascular risk (elevated even at ≤5 mg/day).
- A population cohort found 65% of steroid-treated PMR patients had at least one adverse event, with cumulative doses ≥1,800 mg raising that risk.
The steroid-sparing imperative, plus improved understanding of IL-6 signalling and JAK–STAT biology, has produced a new therapeutic layer — IL-6 receptor inhibitors and JAK inhibitors — reshaping treatment while raising unresolved questions about sequencing, duration, monitoring, and whether any of these agents are truly disease-modifying.
A recurring structural obstacle: treat-to-target (T2T) is conceptually endorsed but hard to operationalise, because there is no validated remission definition and no reliable activity biomarker — a problem worsened by IL-6 blockade, which suppresses CRP/ESR independently of true disease activity.
The review is deliberately split into separate GCA and PMR sections, reflecting real differences in severity, damage risk (vascular in GCA), treatment goals, and evidence strength — while flagging the pathophysiological overlap.
Giant Cell Arteritis — Glucocorticoid Induction
- Standard: oral prednisone 40–60 mg/day for 1–2 weeks, then taper. The optimal starting dose has never been formally tested in an RCT.
- A non-obvious retrospective signal: patients started on >40 mg/day actually reached discontinuation earlier than those on ≤40 mg.
- Alternate-day dosing is inadequate and should not be used.
- IV pulse methylprednisolone (250–1,000 mg/day × 3 days) is reserved for impending or recent visual loss. Its superiority over oral therapy is debated — established ischaemic optic neuropathy is usually irreversible, and pulses add adverse effects (anxiety, insomnia, agitation) in older patients. Not recommended without ischaemic complications.
GCA — Conventional Steroid-Sparing Agents
- Methotrexate: the most rigorously studied conventional agent, but with conflicting RCTs. A meta-analysis of three trials (low-dose MTX 7.5–20 mg) showed a 35% reduction in first relapse and 51% in second relapse, but no reduction in steroid toxicity and a ~6-month lag to effect. Positioned as an alternative when tocilizumab/upadacitinib are unavailable or contraindicated. The METOGiA trial (abstract only) found MTX was not non-inferior to tocilizumab.
- Others are weak or negative: azathioprine (limited benefit), no role for ciclosporin, dapsone/hydroxychloroquine not recommended, leflunomide occasionally used after failure, cyclophosphamide only for refractory life-threatening (e.g. intracranial) disease.
GCA — Antiplatelet / Anticoagulant Therapy
Aspirin’s ischaemia-prevention benefit is unproven (no RCTs). Guidelines discourage routine use, reserving it for independent cardiovascular/cerebrovascular indications or critical vertebral/carotid involvement. A 2025 study (~2,000 patients) found pre-existing anticoagulation — not antiplatelet therapy — associated with fewer cranial ischaemic events.
GCA — IL-6 Receptor Inhibition (the Practice-Changer)
- Tocilizumab (TCZ) is the most studied biologic, FDA/EMA/NICE-approved 2017–2018 on two landmark trials.
- Phase II (n=30): week-12 remission 85% vs 40%; 52-week relapse-free survival 85% vs 20%.
- GiACTA (phase III, n=251): sustained glucocorticoid-free remission at week 52 in 56% (weekly) and 53% (every-other-week) TCZ vs 14%/18% placebo; cumulative prednisone roughly halved (~1,862 mg vs 3,296–3,818 mg). GiACTA also validated a 26-week taper as superior to 52-week steroid monotherapy — hence the 26-week taper recommendation with TCZ.
- Important caveats: ~50% relapse within 1 year of stopping TCZ (long-term tolerance is not restored), persistent vascular inflammation on imaging in one-third to one-half of clinically remitting patients (CRP suppression masks activity), the unresolved question of whether TCZ prevents aneurysm/stenosis, plus dyslipidaemia and diverticulitis/perforation caution.
- Other IL-6 agents (sirukumab, sarilumab) have GCA data but no approval; sarilumab’s trial was COVID-terminated.
- Ultra-short steroid proof-of-concept (GUSTO, TOPAZIO) and 8-week-prednisone studies suggest TCZ can carry much of the load — but these are not standard of care and should be avoided where ischaemia is a concern.
GCA — JAK Inhibition (the Newest Addition)
- SELECT-GCA (2025, phase III, n=428): upadacitinib 15 mg achieved sustained remission 46.4% vs 29.0% placebo, delayed flare, and reduced cumulative steroids (1,615 vs 2,882 mg); the 7.5 mg dose failed. Led to FDA/EMA approval in 2025. The 2-year extension suggests ongoing therapy is needed — remission held only if upadacitinib 15 mg was continued (68.6% vs 28.6%).
- Baricitinib: small open-label pilot, promising, no phase III yet.
GCA — What Has Failed or Disappointed
- Anti-TNF (infliximab, etanercept, adalimumab): no benefit.
- Secukinumab: promising phase II (TitAIN) but failed phase III (GCAptAIN).
- Ustekinumab, guselkumab, anakinra: limited efficacy.
- Mavrilimumab (anti-GM-CSF-R): positive phase II (flares 19% vs 46%), no phase III yet.
- Abatacept: phase II prolonged relapse-free survival (median remission 9.9 vs 3.9 months); phase III ongoing.
GCA — Monitoring and Long-Term Vascular Risk
- Aortic complications matter: up to 17-fold increased thoracic aortic aneurysm risk; aortitis at diagnosis confers ~10-fold higher aneurysm risk. Concerningly, 39% of dissections occurred at aortic width <50 mm — suggesting standard surgical thresholds may not apply in GCA. Baseline aortic imaging is advised; optimal surveillance interval is unsettled.
- Because TCZ suppresses CRP, clinical + imaging assessment (ultrasound, FDG-PET, MRI) matters — though imaging changes lag clinical improvement.
Polymyalgia Rheumatica — Diagnosis and Steroid Induction
- PMR is a diagnosis of exclusion (many mimics: elderly-onset RA, malignancy, infection, GCA). bDMARDs should be withheld until mimics are excluded.
- Standard: prednisone 12.5–25 mg/day, taper to 10 mg by 4–8 weeks, aim to stop within a year — but this typically means ~2 g cumulative steroid, above the harm threshold.
- IM methylprednisolone is an option (less cumulative steroid, fewer fractures) but not widely used.
PMR — Conventional Steroid-Sparing
Methotrexate evidence was historically inconsistent (only 2 of 4 older low-dose trials positive). But a 2026 RCT of MTX 25 mg/week (higher, “proper” dose) with a 24-week taper significantly increased steroid-free remission at 52 weeks — supporting early MTX as a sparing strategy.
PMR — IL-6 Blockade (Now with an Approved Agent)
- Sarilumab is the only agent specifically approved for relapsing PMR (FDA/EMA 2023). SAPHYR (phase III, n=118, COVID-truncated): sustained remission 28.3% vs 10.3%; cumulative steroids markedly lower (777 vs 2,044 mg).
- Tocilizumab data: PMR-SPARE (steroid-free remission at week 16, 63.2% vs 11.8%) and SEMAPHORE in glucocorticoid-dependent PMR (primary endpoint 67.3% vs 31.4%). But relapse after TCZ withdrawal is high (92.3% relapsed, median 15 weeks).
PMR — JAK Inhibition and Other Agents
- Tofacitinib and baricitinib both show strong signals. BATCHELOR (baricitinib): week-12 endpoint 77.8% vs 13.3%, with rescue steroids needed in only 5.6% vs 66.7% — raising the striking possibility of steroid-free PMR management.
- Rituximab: BRIDGE-PMR proof-of-concept suggests possible disease-modifying effect (remission persisted without re-dosing).
- Secukinumab (REPLENISH, abstract): positive in PMR (unlike GCA).
- Infliximab, etanercept: negative.
PMR — Monitoring Pitfalls (the Not-So-Obvious)
- No standard remission/relapse definition; PMR-AS <10 used as a low-activity proxy.
- Inflammatory markers can be normal in relapse: no ESR rise in ~27%, no CRP rise in ~14% — even more relevant under IL-6 blockade.
- Glucocorticoid-induced adrenal insufficiency mimics relapse (below ~7.5 mg/day) — check morning cortisol rather than escalating steroids.
- Subclinical GCA occurs in up to 23% of PMR — consider it in inadequate responders or frequent relapsers.
Key Takeaways
- Glucocorticoids still induce remission in both diseases, but the field has decisively pivoted to steroid-sparing. The goal is no longer just disease control but minimising cumulative steroid toxicity, which is substantial even at low doses.
- IL-6 receptor inhibition is the best-established targeted approach — tocilizumab in GCA (GiACTA) and sarilumab in PMR (the only PMR-specific approval). Both roughly halve cumulative steroids and cut relapse.
- JAK inhibition is the newest tier: upadacitinib is now approved for GCA (SELECT-GCA), and baricitinib/tofacitinib show remarkable steroid-free potential in PMR — though PMR JAK approval is pending and long-term safety in this older population needs more data.
- None of these agents reliably induces durable, treatment-free remission. Relapse after stopping TCZ, upadacitinib, or MTX is common (~half or more), implying these therapies suppress activity without restoring immune tolerance — the disease-modifying question is unanswered.
- Monitoring is a genuine weak point. IL-6 inhibitors suppress CRP/ESR independently of activity; inflammatory markers can be normal in true PMR relapse; and imaging (ultrasound/PET/MRI) both lags clinically and lacks consensus intervals. Clinical assessment remains central.
- Watch the vasculature in GCA long-term: high aneurysm risk, aortitis-at-diagnosis as a red flag, and dissection at sub-threshold aortic diameters — meaning usual surgical cut-offs may under-protect.
- Distinguish PMR from its mimics — and from adrenal insufficiency — before escalating. Subclinical GCA (up to 23%) and steroid-withdrawal adrenal insufficiency are common traps.
- Failed drugs are informative: anti-TNF (both diseases) and secukinumab in GCA (but not PMR) failed — underscoring that GCA and PMR, while overlapping, are not immunologically interchangeable.
- The unresolved agenda: validated remission/biomarker definitions, optimal targeted-therapy duration and tapering, patient selection, cost/access equity, and whether combined GCA–PMR trial designs are viable given their real clinical differences.