Chung M, Shelley JP, Karakoc G, et al. Arthritis Care & Research. 2026;78(5):662–669.
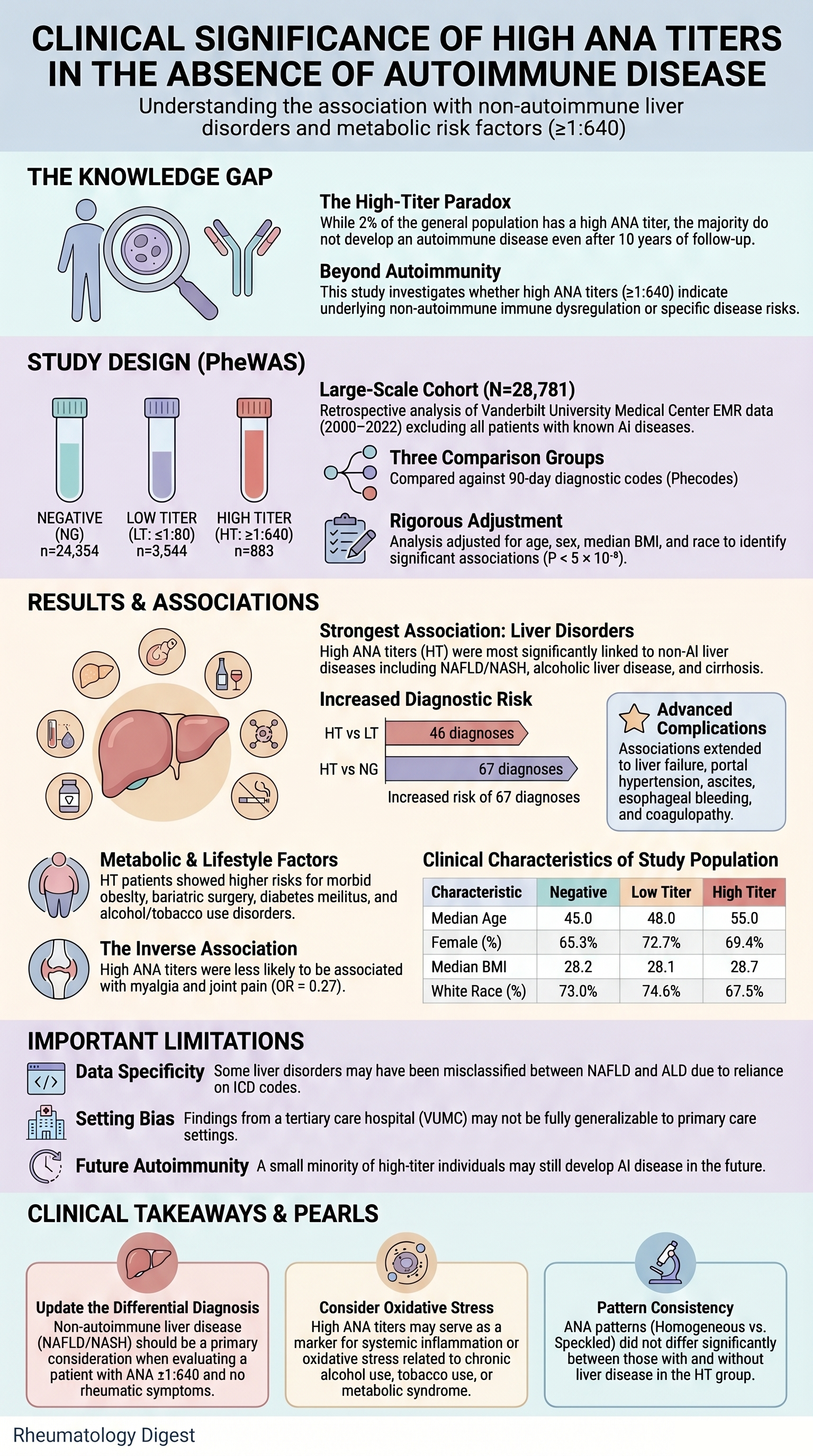
TL;DR: In a 28,781-patient EMR phenome-wide study, a high ANA titer (≥1:640) without autoimmune disease was strongly enriched for non-AI liver disease (NAFLD/NASH, alcohol-related) and metabolic comorbidity — broadening the differential for an unexplained high-titer ANA beyond the usual autoimmune workup.
The Clinical Problem
The antinuclear antibody (ANA) is one of the most frequently ordered rheumatologic tests, yet its interpretation outside the autoimmune (AI) context remains a perennial source of clinical anxiety. While a positive ANA is near-mandatory for SLE (>95% positivity) and is integral to the 2019 EULAR/ACR criteria (which require a titer ≥1:80), high titer ANAs (≥1:640) are found in approximately 2% of the general population — many of whom never develop a classifiable autoimmune disease.
Several questions plague the bedside rheumatologist:
- Does a high ANA titer in a non-AI patient indicate occult immune dysregulation?
- Should such patients be followed indefinitely, reassured, or worked up further?
- Earlier follow-up studies have shown that even at 10 years, only ~6% (2/34) of high-titer ANA individuals without AI disease at baseline went on to develop one — meaning the majority of high titers remain “unexplained.”
Prior literature has linked positive ANAs to cardiovascular events, cancer, infections, and all-cause mortality, but results have been inconsistent. The clinical meaning of a high titer (not just any positive) in a non-autoimmune individual has remained essentially uncharted territory.
The Research Question
Do individuals without autoimmune disease who carry a high ANA titer (≥1:640) show a measurably different burden of clinical diagnoses compared to those with low-titer or negative ANA results?
The authors hypothesized that high titers might reflect immune dysregulation that manifests phenotypically as increased risk for specific (non-AI) conditions — and used a phenome-wide association study (PheWAS) approach to let the data speak without an a priori bias toward any organ system.
How the Study Was Designed
Setting & Design: Retrospective case-control study using Vanderbilt University Medical Center’s (VUMC) de-identified EMR system (Synthetic Derivative/BioVU).
Eligibility:
- Adults (≥18 years) with at least one clinician-ordered ANA test between January 2000 and October 2022.
- ANA performed exclusively by indirect immunofluorescence on HEp-2 cells (per ACR Task Force protocols), using Immuno Concepts or Inova Diagnostics assays.
- Highest titer was selected if multiple ANAs existed.
- Exclusion: any documented ANA-related AI disorder (SLE, Sjögren, SSc, MCTD, AI hepatitis, PBC, idiopathic inflammatory myopathies, etc.) — at any time point in the EMR, not just before testing.
Group Allocation: Three mutually exclusive cohorts —
- High titer (HT): ANA ≥ 1:640
- Low titer (LT): ANA ≤ 1:80
- Negative (NG): Only negative ANA results
- Intermediate titers (1:80 < titer < 1:640) were deliberately excluded to sharpen the contrast.
Phenotyping Approach (the technical heart of the study):
- ICD-9 and ICD-10 codes were mapped to Phecodes (v1.2) — these aggregate related ICD codes into clinically meaningful disease entities.
- Cases = ≥2 occurrences of a Phecode in the EMR; Controls = absence of that Phecode or any closely related Phecode.
- Only diagnoses first recorded within ±90 days of the ANA test were counted — a clever design choice meant to reduce contamination by long-standing prevalent disease.
- Phecodes with <100 cases were dropped to preserve statistical power.
- Adjustments: age at ANA testing, sex, median BMI (15–60 kg/m² range), and reported race.
- Significance threshold: P < 5 × 10⁻⁵ (a Bonferroni-style correction for the large number of Phecodes tested).
Case Validation: For the 10 most significant associations, 50 random charts were manually reviewed to compute the positive predictive value (PPV) of the Phecode-based phenotype.
The Study Population
From an initial pool of 88,501 individuals with ANA tests:
- 45,624 were excluded for established AI disease
- 4,700 lacked BMI data
- 8,488 had intermediate titers (excluded by design)
- 908 had no diagnostic code within ±90 days
Final cohort: 28,781 individuals
| Group | n | % | Median Age (IQR) |
|---|---|---|---|
| Negative (NG) | 24,354 | 84.6% | 45 (33–56) |
| Low titer (LT) | 3,544 | 12.3% | 48 (37–60) |
| High titer (HT) | 883 | 3.1% | 55 (42–66) |
Key observations on baseline characteristics:
- HT patients were significantly older (P = 3.9 × 10⁻⁷³), consistent with the known age-related rise in ANA prevalence.
- Female predominance across all groups (65–73%).
- BMI did not differ between groups (P = 0.345) — an important null finding that becomes interesting later.
- ANA patterns (available in 95.8% of HT vs only 23.4% of LT): Homogeneous (~57%) and Speckled (~38%) dominated. Nucleolar was ~3–5%. No striking pattern enrichment differentiated HT from LT.
The Results
Comparison 1 — HT vs LT (46 significant Phecode associations):
The top hits were overwhelmingly hepatic and metabolic:
- Chronic liver disease (Phecode 571)
- NAFLD / NASH (Phecode 571.5)
- Alcohol-related liver disease (Phecode 317)
- Cirrhosis (non-alcoholic), alcoholic liver damage, portal hypertension, ascites, esophageal varices/bleeding, liver abscess
- Surrogates of severe liver disease: coagulation defects, thrombocytopenia, hyponatremia, acidosis, protein-calorie malnutrition, hepatic encephalopathy markers (altered mental status)
- Metabolic correlates: obesity, overweight, diabetes mellitus
- Behavioral/psychiatric: alcoholism, tobacco use disorder, anxiety, mood disorders
- An interesting finding: Pain (Phecode 338) was more common in HT (OR 4.1, P = 1.9 × 10⁻¹³), but myalgia (Phecode 770) was less common (OR 0.27, P = 1.3 × 10⁻⁵) — a likely reflection of referral and screening bias (myalgic patients with high ANA tend to get an AI label and would have been excluded).
Comparison 2 — HT vs NG (67 significant associations):
- 59 of the 67 overlapped with the HT vs LT findings.
- New associations: biliary tract disorders (cholelithiasis, cholecystitis), GI disorders (hemorrhoids, esophageal disease), bariatric surgery, insulin pump use, screening for skin malignancy, and poisoning by antibiotics, anti-infectives, and analgesics/antipyretics/antirheumatics (likely reflecting hepatotoxicity events in patients with underlying liver disease).
Case Validation (the credibility check):
- For Phecode 573 (“Other disorders of the liver”): PPV = 88% for non-AI liver disease.
- Fatty liver disease was the most common etiology, followed by alcohol and hepatitis C.
- Only 3/50 charts had possible undiagnosed AI liver disease (PBC or AIH) — i.e., the signal is not explained by missed autoimmune hepatitis.
- For alcohol-related Phecodes (317.1, 317.11): PPV = 92% for genuine alcohol-attributable disease.
Sensitivity analyses:
- Excluding BMI as a covariate did not alter the conclusions.
- Among HT individuals, ANA patterns did not differ between those with and without liver disease — so no single immunofluorescent pattern is acting as a “tag” for hepatic disease.
Study Limitations
The authors are commendably forthcoming. The key caveats:
- Phenotype misclassification — Phecodes derived from ICD codes can over- or under-call diagnoses; mitigated (but not eliminated) by the 88–92% PPVs.
- Future AI disease — some HT individuals may develop AI disease later; excluding ever-diagnosed AI patients reduces but does not eliminate this.
- Incident vs prevalent disease — the ±90 day window helps, but patients newly enrolled at VUMC may have brought chronic diagnoses with them.
- Single-center, tertiary referral cohort — generalizability to community settings is uncertain.
- Pre-ICAP era testing — most ANAs predate the International Consensus on ANA Patterns (ICAP, 2019) recommendations, so pattern reporting was less standardized.
- DFS70 not assessed — these antibodies (dense fine speckled pattern) are notoriously difficult to detect by HEp-2 IIF alone and require solid-phase confirmation. They are associated with the absence of systemic AI disease, and whether DFS70 positivity drives some of the signal here remains unknown.
- Causality cannot be inferred — does the high ANA reflect underlying liver disease, or does the immune dysregulation drive both? PheWAS cannot disentangle this.
How This Study Adds to Practice
This is the first large-scale, hypothesis-free evaluation of what a high ANA titer means in patients without autoimmune disease. The clinical implications:
- Non-autoimmune liver disease deserves a formal place in the differential of an unexplained high-titer ANA. Currently, most algorithms emphasize AI hepatitis or PBC; this study shows NAFLD/NASH and alcoholic liver disease are quantitatively more important explanations.
- The mechanism likely involves oxidative stress — chronic alcohol, tobacco, and lipotoxicity all generate reactive species and neoantigens (e.g., malondialdehyde-acetaldehyde adducts) that can drive autoantibody production without triggering full-blown AI disease.
- The signal extends beyond liver involvement itself to its complications — cirrhosis, portal hypertension, varices, ascites, coagulopathy. This raises the question of whether high ANA titers might be a marker of progression in NAFLD, although the cross-sectional design cannot confirm this.
- Metabolic comorbidity matters — despite similar median BMI across groups, the distribution skewed toward obesity in HT patients (twice the proportion in overweight/obese categories), and bariatric surgery and insulin pump use were enriched. The “inverse BMI-ANA association” seen in some prior epidemiologic studies may be confounded by NAFLD-driven cases.
- For the rheumatologist: when you encounter a referral for a “high ANA without symptoms,” consider checking LFTs, asking about alcohol use, and screening for metabolic syndrome / NAFLD risk factors before committing to indefinite serial autoimmune workups.
Final Takeaways
- A high ANA titer (≥1:640) in a person without autoimmune disease is not biologically silent — it is statistically enriched for liver disease (NAFLD/NASH, ALD) and its sequelae.
- The Phecode-based PheWAS approach offers a powerful, hypothesis-free way to interrogate large EMR datasets, and the manual chart validation (PPV 88–92%) lends credibility to the top associations.
- The mechanistic thread is plausibly oxidative stress → autoantibody generation in the setting of chronic hepatic and metabolic injury.
- Rheumatologists should broaden the differential for an unexplained high-titer ANA to include hepatic and metabolic disorders. Reflexively repeating ANAs or pursuing exhaustive AI workups in such patients may be lower-yield than a focused hepatology evaluation.
- Open questions for the field:
- Does the high ANA predict progression of NAFLD to fibrosis?
- What is the role of DFS70 in this population?
- Is there value in serial ANA monitoring in liver disease patients?
- Can the immunologic phenotype of these patients be reversed by treating the metabolic/hepatic driver?
A useful one-liner for clinic: An ANA of 1:640 in a healthy-looking patient may be a quiet flag for an unhealthy liver — check the LFTs before you check the dsDNA.