TL;DR: IL-5 blockade has transformed EGPA care — mepolizumab and benralizumab both improve remission, cut relapses >40% and deliver major glucocorticoid-sparing, with benralizumab noninferior to mepolizumab and possibly enabling fuller steroid withdrawal — but the trial evidence is skewed to the eosinophilic-asthmatic phenotype, leaving control of the vasculitic compartment unproven.
The Clinical Problem
EGPA is an ANCA-associated vasculitis defined by eosinophil-driven inflammation. Historically, control depended on glucocorticoids (GC) with or without conventional immunosuppressants, leaving many patients GC-dependent, relapsing, or refractory, and exposed to cumulative steroid toxicity. Because IL-5 is the master cytokine governing eosinophil differentiation, activation and survival, and because serum IL-5 tracks disease activity, the IL-5 axis became a logical therapeutic target. The review synthesises the biology of IL-5/eosinophils and the trial and real-world evidence for the two approved IL-5 pathway inhibitors — mepolizumab (anti–IL-5) and benralizumab (anti–IL-5Rα) — while mapping the remaining unmet needs.
IL-5 Biology and the Eosinophil Life Cycle
- IL-5 acts on four eosinophil functions: differentiation, migration, activation, survival. It does not commit the lineage but, via IL-5Rα on marrow progenitors, drives proliferation and maturation.
- Migration depends on the β2-integrin CD11b/CD18, induced by IL-5 through the MAPK pathway, enhancing adhesion to endothelium.
- IL-5 prolongs eosinophil survival by blocking apoptosis (notably via Bid inactivation in the Fas pathway). Circulating eosinophil half-life is normally <24 hours.
- Signalling runs through JAK2/STAT5 (essential in mice) plus MAPK, with Lyn and BTK also involved — the mechanistic rationale for exploring JAK inhibition.
- Produced by Th2 cells, ILCs, mast cells, basophils and dendritic cells; eosinophils remain the dominant effector cell.
Eosinophils in EGPA
- Normal blood eosinophils: 100–400 × 10⁶/L; hypereosinophilia = persistent elevation >1,000–1,500 × 10⁶/L. The 2022 ACR/EULAR classification criteria use a 1,000 × 10⁶/L cut-off.
- In health, >90% of eosinophils are tissue-resident (rEOS). A less obvious point: emerging flow phenotyping distinguishes inflammatory iEOS (Siglec8⁺CD16⁻CD62L^low) from resident rEOS (CD62L^high) — iEOS correlate with asthma/sinusitis activity and are reduced by anti–IL-5 therapy. Not yet routine clinically.
- Tissue damage mechanisms: granule proteins (major basic protein, EPO, ECP), activation of coagulation via tissue factor, and ETosis releasing galectin-10 that crystallises into Charcot-Leyden crystals — a hallmark of eosinophilic inflammation.
- Pathogenic dichotomy worth emphasising: ANCA-positive EGPA is HLA-linked (HLA-DQ), adaptive/autoantibody-driven, with neutrophil-mediated small-vessel vasculitis. ANCA-negative EGPA associates with IL-5, IRF1, GATA3 polymorphisms — i.e. barrier dysfunction and eosinophil activation dominate, often with subtle or absent histologic vasculitis.
The Diagnostic Trap: EGPA vs HES
ANCA-negative EGPA vs hypereosinophilic syndrome (HES) is the hardest differential — both show peripheral hypereosinophilia (≥1,500 × 10⁶/L) and eosinophil-mediated organ damage. Discriminators:
- Favouring EGPA: CRSwNP, asthma, mononeuritis multiplex, palpable purpura; eosinophil-rich necrotising granulomatous vasculitis on biopsy.
- Favouring HES: eosinophilic myocarditis/gastroenteritis, varied non-purpuric skin disease; typically no granulomas or vasculitis.
- Workup in ANCA-negative chronic hypereosinophilia: ANCA, vitamin B12 (raised in myeloproliferative HES), FIP1L1-PDGFRA and other tyrosine-kinase fusions, plus parasitic screens (Strongyloides, Toxocara).
- The two can coexist or evolve — a reason for ongoing follow-up and diagnostic reconsideration.
The IL-5 Pathway Inhibitors — Mechanism Matters
- Mepolizumab, reslizumab, depemokimab neutralise circulating IL-5.
- Benralizumab binds IL-5Rα and additionally recruits NK-cell ADCC, producing near-total eosinophil depletion. In asthma it depleted 95.8% airway, 89.9% sputum, 100% bone marrow eosinophils, versus ~50% tissue depletion for mepolizumab in eosinophilic oesophagitis. Whether this deeper depletion is clinically superior — or risks depleting protective rEOS — is unknown.
- Approved EGPA dosing: mepolizumab 300 mg SC q4w (≥6 years); benralizumab 30 mg SC q4w (≥18 years). The 300 mg mepolizumab dose was justified by a 16-study dose–response meta-analysis for high-BEC diseases (>1,000 cells).
Trial Evidence
MIRRA (Wechsler, NEJM 2017): mepolizumab 300 mg q4w vs placebo, 52 wks, n=68/arm, relapsing/refractory GC-dependent EGPA.
- ≥24 weeks of accrued remission: 28% vs 3%.
- Remission at wks 36 & 48 (BVAS=0, PDN ≤4 mg): 32% vs 3%; by EULAR definition (≤7.5 mg): 41% vs 10%.
- Relapse frequency reduced >40%; relapse-free survival 44% vs 18%.
- GC-sparing: PDN ≤4 mg in final 4 wks 44% vs 7%; off PDN 18% vs 3%; cumulative PDN 1,423 mg lower.
- BEC: 83% lower than placebo by week 4.
- Caveat: only 10% ANCA-positive, ~5-year disease duration, predominantly eosinophilic-asthmatic (not vasculitic) phenotype.
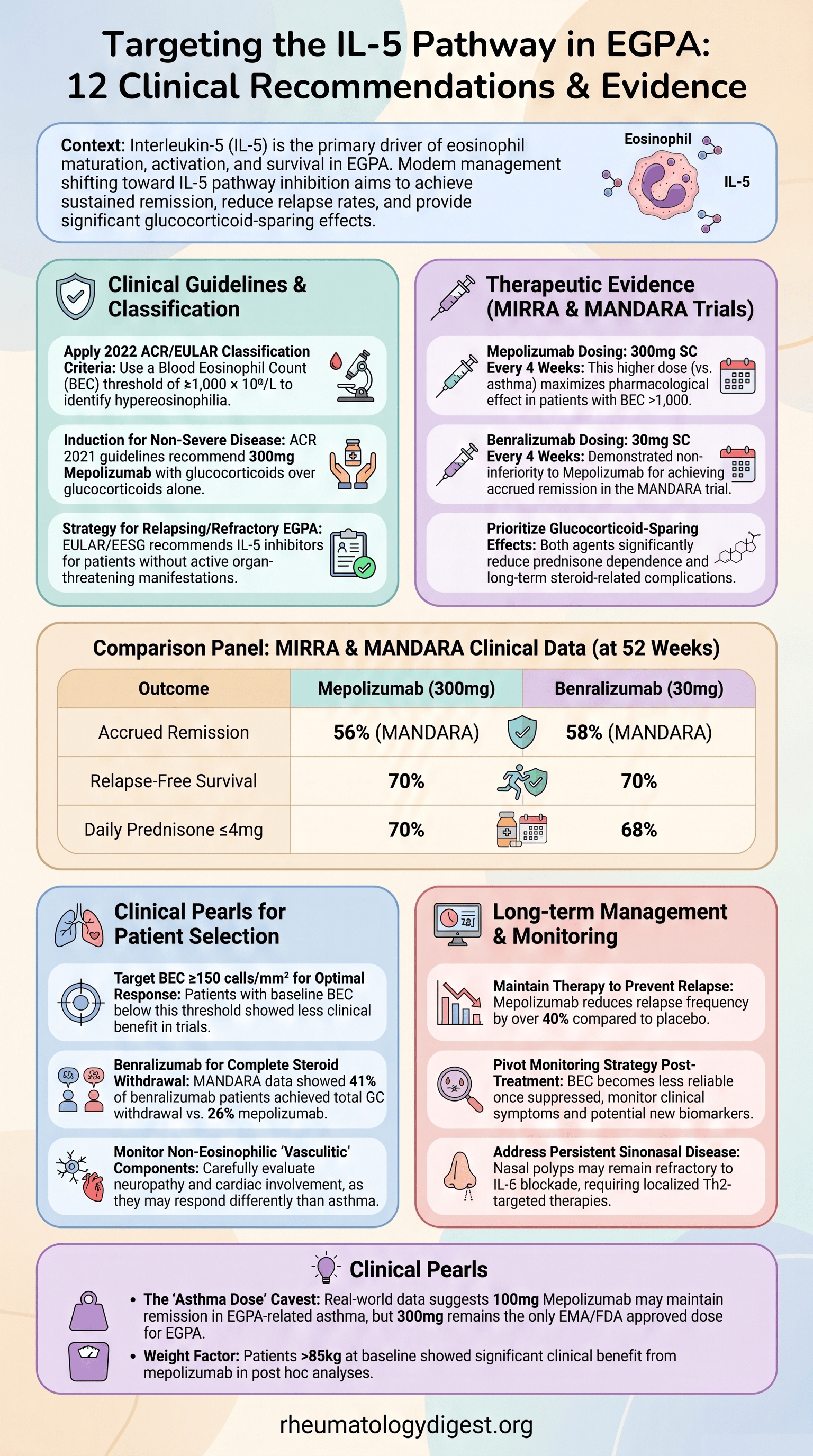
MANDARA (Wechsler, NEJM 2024): benralizumab 30 mg vs mepolizumab 300 mg, 52 wks, noninferiority, n=70/arm.
- Remission wks 36 & 48: benra 58% vs mepo 56% (trial def); 79% vs 74% (EULAR def) — noninferiority met, superiority not.
- ~30% relapsed in each arm.
- Complete GC withdrawal: benralizumab 41% vs mepolizumab 26% (wks 48–52) — consistent with benralizumab’s deeper depletion.
- BEC reduction greater/faster with benralizumab (week 1: 85% vs 61%; week 52: 90% vs 74%).
- Post hoc (abstract): 4-component asthma remission 28.0% (benra) vs 12.4% (mepo).
- Same caveat: ~10% ANCA-positive, asthmatic-predominant.
Non-obvious nuance: mepolizumab’s GC-sparing numbers look much better in MANDARA than in MIRRA (≤4 mg PDN 70% vs 44%) — attributed to differing trial designs, not a true drug change. Cross-trial comparisons should therefore be made cautiously.
Real-World Data
- Both drugs confirmed effective and steroid-sparing even at the lower “asthma doses” (mepolizumab 100 mg q4w; benralizumab 30 mg q8w), with GC-free remission in >65% in one benralizumab series.
- Benralizumab showed lower efficacy after prior mepolizumab failure, and numerically higher discontinuation than mepolizumab (18% vs 10%).
- No consensus yet on dose-tapering by BEC or clinical control.
Guidelines (Note the Timing Gap)
- 2021 ACR/VF: mepolizumab 300 mg q4w added to GC for active non-severe EGPA.
- 2022 EULAR / EESG: mepolizumab for induction in relapsing/refractory non–organ-threatening EGPA, and for maintenance.
- Benralizumab appears in no guideline — MANDARA published early 2024, after all current recommendations.
- No trial has tested any anti–IL-5 agent as first-line therapy in newly diagnosed EGPA.
Predictors of Response
- Mepolizumab benefit was largely independent of baseline BVAS, VDI ≥5, ANCA status, refractory disease, immunosuppressant use, EGPA duration >4 yrs, or prior relapses.
- Two signals did emerge: baseline BEC ≥150 cells/mm³ (≥24-wk remission 33% vs 0% with placebo; no benefit if <150) and weight >85 kg.
- No validated predictors for benralizumab; real-world data show no ANCA-status difference.
Key Takeaways
- IL-5 blockade has transformed EGPA care — both mepolizumab and benralizumab improve remission, cut relapses >40%, and deliver major glucocorticoid-sparing. Benralizumab is noninferior to mepolizumab and may achieve fuller steroid withdrawal owing to NK-mediated eosinophil depletion.
- The evidence base is skewed toward the eosinophilic-asthmatic phenotype. Trial populations were ~90% ANCA-negative with long disease duration; whether anti–IL-5 therapy controls the vasculitic compartment (vasa nervorum neuropathy, GI vasculitis, coronaritis) remains unproven.
- Two persistent therapeutic gaps: refractory sinonasal disease/nasal polyps (dupilumab helps CRSwNP but triggered systemic flares in ~⅓), and the unknown impact of IL-5 inhibition on cardiovascular/thrombotic risk.
- Biomarker challenge of success: as anti–IL-5 therapy normalises BEC, eosinophil count loses value as an activity marker. Urine eosinophil-derived neurotoxin (uEDN) is a promising activity biomarker that stays informative under treatment.
- Pipeline to watch: JAK1 inhibitor (NS-229, NCT06046222), anti-TSLP tezepelumab (RACEMATE, NCT06230354) for upstream/IL-5–independent disease, and long-acting depemokimab (OCEAN, NCT05263934, q26w dosing). Sequential/combination strategies (e.g. rituximab→mepolizumab) are being explored for mixed eosinophilic-vasculitic phenotypes.
- Open practical question: no head-to-head of mepolizumab 100 mg vs 300 mg, and no consensus on BEC- or symptom-guided de-escalation after sustained control.