Allenbach Y, Benveniste O. N Engl J Med 2026;394:1925-38
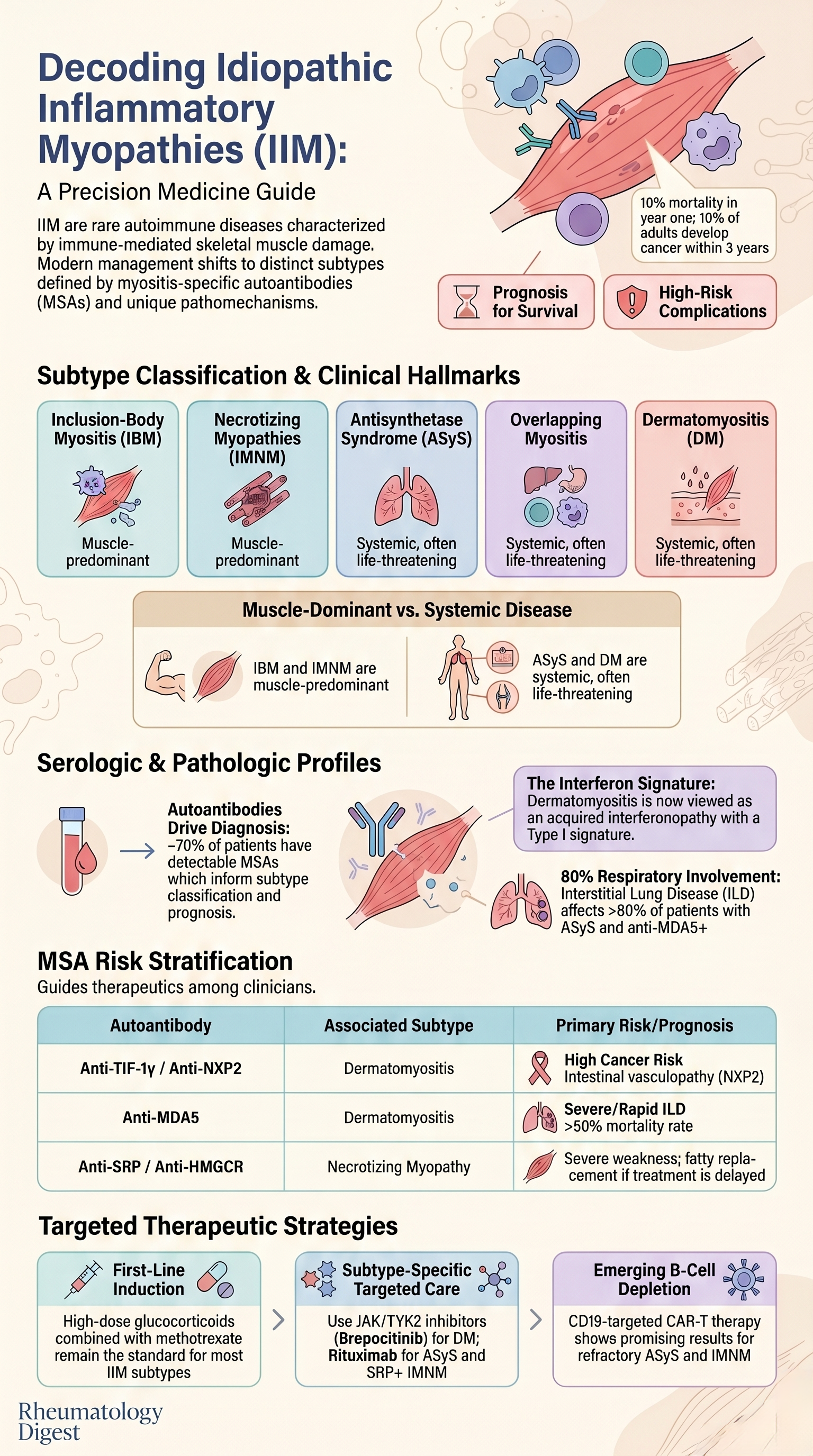
TL;DR: Five subtypes (IBM, IMNM, antisynthetase syndrome, overlap, dermatomyositis), anchored by myositis-specific autoantibodies, now define the inflammatory myopathies — each with its own organ involvement, cancer risk, prognosis, and increasingly subtype-targeted therapy. The clinical task is no longer to recognise myositis, but to subclassify it.
The Clinical Problem
Idiopathic inflammatory myopathies (IIMs) are a rare, heterogeneous group of autoimmune disorders characterised by immune-mediated injury to skeletal muscle, often with systemic involvement. Although historically lumped together as “polymyositis” or “dermatomyositis,” our understanding has evolved dramatically. The challenge for the clinician is no longer simply recognising myositis, but accurately subclassifying it — because each subtype has a distinct natural history, organ involvement, prognosis, cancer risk, and therapeutic response. Misclassification can mean missing a life-threatening interstitial lung disease (ILD), failing to screen for an associated malignancy, or prescribing steroids that will not work (as in inclusion-body myositis).
The epidemiological footprint is small but clinically important: incidence ~0.79/100,000 person-years; prevalence ~14/100,000. Female predominance is the norm — except for inclusion-body myositis (IBM), which favours men over 35 years (peak ~60 years). Heritability reaches ~24% in identical twins, with HLA being the dominant susceptibility locus, but environmental triggers (infection, UV light, smoking, statins, malignancy) clearly contribute.
What the Paper Explains
The review consolidates the modern five-subtype classification of IIM, anchored by myositis-specific autoantibodies (MSAs) and myopathological patterns, and traces how this has translated into targeted therapeutics.
The Five Subtypes — A Quick Anchor
- Inclusion-body myositis (IBM)
- Immune-mediated necrotizing myopathy (IMNM)
- Antisynthetase syndrome (ASyS)
- Overlapping myositis (in the context of systemic sclerosis, MCTD, etc.)
- Dermatomyositis (DM)
“Polymyositis” as a standalone entity is now considered rare — most cases reclassify into one of the above once MSAs and biopsy are scrutinised.
Clinical Features — Subtype Fingerprints
Muscle Involvement Patterns
IBM: Slowly progressive, asymmetric weakness; the quadriceps + finger flexors distribution is almost pathognomonic. CK normal to moderately elevated (often 2–4× ULN). MRI: inflammation plus fatty replacement in deep finger flexors and quadriceps.
IMNM: Rapidly progressive, symmetric, primarily lumbopelvic weakness. Very high CK (often 20–30× ULN). MRI: T2 hyperintensity (active inflammation) in pelvifemoral muscles; T1 hyperintensity (fatty replacement) when treatment is delayed.
ASyS: Symmetric, proximal, subacute, moderate weakness despite CK 10–20× ULN. Importantly, ~1/3 of ASyS patients never develop myositis — they present with ILD or arthritis instead.
DM: Symmetric proximal weakness, deltoids affected first. CK may be normal and does not correlate with weakness. At least 1/3 are amyopathic (skin-dominant with little/no muscle involvement).
Extramuscular Features (key for DM and ASyS)
Skin lesions in DM:
- Heliotrope rash (eyelids/periorbital)
- Gottron’s papules (MCP, PIP joints) and Gottron’s sign (elbows, knees)
- V sign (anterior chest), shawl sign (upper back), holster sign (lateral thighs)
- Scalp involvement, alopecia
- Dermatomyositis sine dermatitis in ~8% — often anti-NXP2 positive
- Severe vasculopathy with skin ulcers → think anti-MDA5
- Mechanic’s hands → suggests ASyS (or anti-MDA5 DM)
- Raynaud’s phenomenon — DM and ASyS
Organ involvement (approximate frequencies):
- Dermatologic ~40% (nearly universal in DM)
- Respiratory ~40% — ILD in >80% of ASyS and anti-MDA5 DM
- Digestive ~30% (dysphagia dominant)
- Joints ~20% (non-erosive polyarthritis in ASyS, overlap, anti-MDA5 DM)
- Oncologic ~15%
- Cardiac ~5% (rare but life-threatening)
IBM and IMNM are essentially muscle-only — extramuscular features are not seen.
Diagnosis and Classification
The Autoantibody Revolution
- ~70% of myositis patients have detectable autoantibodies
- ~30 MSAs identified; they are largely mutually exclusive
- MSAs now inform diagnosis, subtype, prognosis, cancer risk, and treatment
DM-specific autoantibodies: anti-Mi-2, anti-TIF-1γ, anti-SAE, anti-NXP2, anti-MDA5
ASyS-specific (8 known; anti-Jo-1, anti-PL-7, anti-PL-12 account for >90%)
IMNM-specific: anti-SRP, anti-HMGCR
IBM: anti-cN1A (present but not specific — also seen in Sjögren’s, SLE, and individuals without muscle disease)
Myositis-associated antibodies (seen in overlap syndromes): anti-Ro52/Ro60, anti-U1RNP, anti-Ku, anti-PM/Scl
Important Caveats on Testing
- Standard HEp-2 ANA screening misses many MSAs — multiplex immunoassays are needed.
- Some assays are less reliable (anti-TIF-1γ, anti-SAE, anti-EJ, anti-OJ, anti-Zo, anti-cN1A) — clinical-biopsy correlation is essential.
- Repeat testing with reference methods when results don’t fit the clinical picture.
Role of Biopsy
Muscle biopsy is no longer mandatory when the clinical–serological picture is clear, but remains essential for:
- All suspected IBM cases
- Seronegative patients
- Ruling out mimics (dystrophies, drug-induced, infectious, hypothyroid myopathy)
Skin biopsy is a useful alternative in MSA-negative amyopathic DM (shows vasculopathy + interface dermatitis).
Characteristic Biopsy Patterns
- IBM: Vacuolated/tunnelized fibres surrounded by lymphocytes; endomysial inflammation
- IMNM: Minimal inflammation; randomly distributed necrotic fibres at various stages (early hyalinized → macrophage-cleared)
- ASyS: Perifascicular necrosis with perimysial inflammatory infiltrates and perivascular inflammation
- DM: Perifascicular atrophy (not necrosis); vasculopathy with endocapillary C5b-9 deposition
Differential Diagnosis Pearls
- Young patient (<30 y), high CK, no MSA → consider genetic myopathies (dysferlinopathy, FSHD can both show inflammatory infiltrates)
- No response to steroids → reconsider IBM or hereditary myopathy
- Subacute onset → exclude statin-induced (without anti-HMGCR), hypothyroidism, infections (HIV, trichinellosis, leptospirosis)
Prognosis
Survival
- ~10% mortality in the first year after diagnosis
- Leading causes of death: cancer and respiratory complications (pulmonary fibrosis, pulmonary hypertension)
- ~10% of adults develop cancer within 3 years before or after diagnosis
High cancer risk (warrants intensive screening):
- Anti-TIF-1γ, anti-NXP2, seronegative DM (especially age >40), anti-OJ ASyS
Low cancer risk:
- IBM, ASyS (mostly), overlap myositis, Raynaud’s phenomenon, anti-Jo-1, anti-SRP
ILD-Driven Mortality
- ASyS 10-year survival: 70% in anti-Jo-1 positive vs 47% in non-Jo-1 (PL-7, PL-12, EJ, KS, OJ)
- Anti-MDA5 DM: rapidly progressive ILD in ~30%; mortality >50%
Functional Prognosis
- Worst muscle outcomes: untreated IMNM and IBM (progressive fatty replacement)
- IBM typically requires walking aids within 10 years of diagnosis
- DM and ASyS muscle deficits often improve substantially with treatment
- Joint disease in ASyS/overlap is generally non-erosive
Pathophysiology — Why Each Subtype Responds Differently
Transcriptomic analysis confirms four distinct molecular signatures:
IBM — dual mechanism: autoimmune (oligoclonal, terminally differentiated CD8+ T cells; IFN-γ-rich milieu) + degenerative (rimmed vacuoles, protein aggregates, ER stress, autophagy/mitochondrial dysfunction). Recent xenograft data suggest degeneration can progress independently of immunity — explaining steroid resistance.
IMNM — necrotic fibres with endomysial macrophage infiltrates; sarcoplasmic fine granular p62 pattern. Anti-HMGCR antibodies are internalised into myofibres and inhibit HMGCR activity in vitro, leading to lipid droplet accumulation and necrosis. Genetic HMGCR loss-of-function causes a similar phenotype — strong evidence for antibody pathogenicity. CAR-T success further supports a B-cell pathogenic role.
ASyS — Perifascicular necrosis with T-cell, B-cell, and plasma-cell niches. Animal models support a pathogenic role for the humoral anti-Jo-1 response, particularly in lung tissue.
DM — A type I interferonopathy: prominent IFN-β signature in muscle, skin, and blood; cytotoxic to muscle and endothelial cells. All DM-specific antibodies target proteins within the interferon pathway. Genetic interferonopathies produce similar vasculopathy — supporting the “acquired interferonopathy” model.
Treatment — Now Subtype-Targeted
Inclusion-Body Myositis
- No proven disease-modifying therapy.
- IVIG, steroids, methotrexate — ineffective and may worsen weakness.
- Recent failures: arimoclomol and bimagrumab (both negative in large trials).
- Sirolimus showed negative primary but positive secondary endpoints → phase 3 ongoing (NCT04789070).
- Anti-KLRG1 (targeting terminally differentiated effector T cells) — phase 2–3 completed.
Immune-Mediated Necrotizing Myopathy
- High-dose glucocorticoids + methotrexate is the standard.
- Anti-HMGCR: add IVIG
- Anti-SRP: consider rituximab
- CAR-T (CD19) shows promise in refractory cases
Antisynthetase Syndrome
- B-cell depletion (rituximab) — increasingly favoured, especially for ILD
- Mycophenolate, azathioprine, cyclophosphamide, calcineurin inhibitors for ILD
- CAR-T shows promising early results, even in severe ILD
Rapidly Progressive ILD (anti-MDA5 DM and some ASyS)
- Triple therapy: high-dose steroids + cyclophosphamide + calcineurin inhibitor (most common combination)
- Alternatives include JAK inhibitors, rituximab, mycophenolate
- Rituximab benefit is delayed — may not suit fulminant cases
- Lung transplantation is an option in refractory disease
Dermatomyositis
- Steroids + methotrexate (extrapolated from juvenile DM trial showing better tolerability than ciclosporin)
- IVIG: the only regulator-approved therapy for DM (phase 3 trial by Aggarwal et al.)
- JAK inhibitors (NCT04972760) and TYK2 inhibitors (NCT05695950) under trial
- Brepocitinib (dual TYK2–JAK1 inhibitor) — significant benefit shown in a phase 3 trial reported in the same NEJM issue (Vleugels et al.)
- Anti-IFN type I receptor and anti-IFN-β monoclonals in trials
Universal Recommendation
- Combined aerobic + resistance exercise, 3×/week is beneficial across all subtypes — improves endurance, strength, and quality of life.
Therapeutic Frontiers
- FcRn blockade (efgartigimod-like agents) to reduce autoantibody half-life — trials in IMNM, ASyS, DM (NCT05523167, NCT05379634)
- Daratumumab (anti-CD38, plasma cell depletion) — success in refractory anti-SRP IMNM and anti-MDA5 DM
- Anti-CD19 CAR-T: promising across IMNM, ASyS, and even juvenile DM
- Nintedanib for myositis-associated ILD (NCT05799755)
Key Takeaways for the Rheumatologist
Abandon “polymyositis” as a working diagnosis. Most cases reclassify with proper MSA testing and biopsy. The five-subtype framework (IBM, IMNM, ASyS, overlap, DM) is the modern standard.
MSA testing is essential, but interpret in clinical context. Multiplex immunoassays are required (HEp-2 ANA misses MSAs). Some assays (anti-TIF-1γ, anti-SAE, anti-OJ, anti-cN1A) have reliability issues — verify when results don’t fit.
Match the clinical fingerprint to the subtype:
- Asymmetric, finger flexor + quadriceps weakness → think IBM
- Very high CK, rapid lumbopelvic weakness → think IMNM
- Moderate weakness + ILD + arthritis + mechanic’s hands → think ASyS
- Rashes ± weakness → think DM; severe skin ulcers + ILD → think anti-MDA5
Cancer screening is risk-stratified by MSA. Intensive screening for anti-TIF-1γ, anti-NXP2, anti-OJ, and seronegative DM (especially >40 y). Lower-risk groups need standard age-appropriate screening only.
ILD drives mortality in ASyS and anti-MDA5 DM — screen proactively (HRCT), and remember that ~1/3 of ASyS patients have no myositis at all.
Steroid non-response should prompt reconsideration — think IBM, genetic myopathy, or wrong diagnosis.
Therapy is now subtype-specific:
- IBM has no effective DMT yet — counsel honestly
- IMNM → steroids + MTX, with IVIG for anti-HMGCR and rituximab for anti-SRP
- ASyS → strong case for early rituximab, especially with ILD
- DM → steroids + MTX + IVIG, with JAK/TYK2 inhibitors emerging
- Rapidly progressive ILD → aggressive triple therapy upfront
Exercise is therapy — combined aerobic + resistance training 3×/week should be part of every management plan.
The next decade belongs to targeted biologics: FcRn blockers, JAK/TYK2 inhibitors, anti-CD19 CAR-T, daratumumab, and IFN-pathway agents are reshaping the field — many likely to enter rheumatology practice imminently.
Biopsy remains the gold standard when the picture is unclear, when MSAs are negative, and always for IBM. Skin biopsy is a valuable alternative in amyopathic DM.
A practical mental model: ask first “is this muscle-only (IBM/IMNM) or systemic (DM/ASyS/overlap)?” Then let the MSA refine the subtype, predict the organ involvement, stratify cancer risk, and choose the therapy.