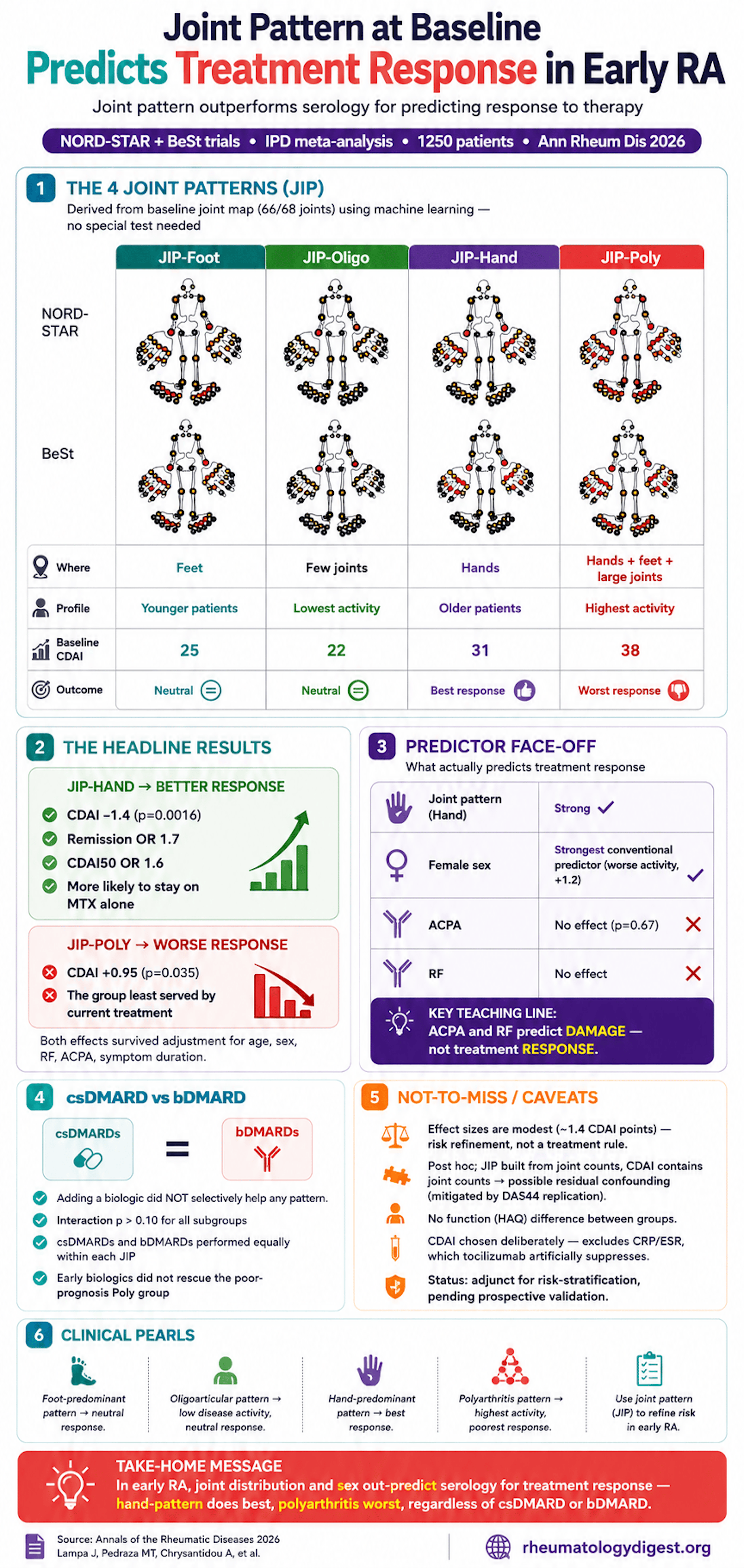
TL;DR: In early RA, where the arthritis is distributed predicts treatment response — hand-dominant disease (JIP-Hand) does better and polyarthritis (JIP-Poly) worse, independent of sex and serology and equally across csDMARDs and bDMARDs — while ACPA/RF (damage markers) show no association with short-term disease-activity response and female sex outperforms them as a predictor.
The Clinical Problem
Rheumatoid arthritis is heterogeneous — in phenotype and, more frustratingly, in treatment response. Clinicians want to know at baseline who will do well on standard therapy and who will not, but the tools available are weak:
- ACPA and RF predict long-term radiographic damage, but are only weakly (if at all) predictive of short-term disease-activity response to treatment.
- Worse, ACPA, RF, and high disease activity are all baked into the 2010 ACR/EULAR classification criteria, so most early RA patients carry at least one “poor-prognostic” marker — which makes them useless for separating patients.
So there is a real need for a novel, routinely available predictor of treatment response.
The authors’ prior work used deep learning + clustering on baseline joint distribution (66/68 joint scheme) to derive four reproducible “joint involvement pattern” (JIP) subgroups: JIP-Foot, JIP-Oligo, JIP-Hand, JIP-Poly. In their original cohort, JIP-Hand had better MTX retention and remission. This study asks whether that signal holds up in independent trial data.
The Research Question
In treatment-naïve early RA, do the four JIP subgroups predict disease-activity response to treatment — and does the effect differ between csDMARDs and bDMARDs? Secondarily, how does JIP compare against conventional predictors (age, sex, RF, ACPA, symptom duration)?
How the Study Was Designed
Design: One-stage IPD meta-analysis pooling two RCTs of treatment-naïve early RA — NORD-STAR (n=812, Nordic + Netherlands, 2010 criteria) and BeSt (n=508, Netherlands, older 1987-criteria trial). Combined 1250 patients.
The two trials differ usefully:
- NORD-STAR: all arms MTX-based; arm 1 active conventional (± prednisolone or SSZ+HCQ), arm 2 certolizumab, arm 3 abatacept, arm 4 tocilizumab.
- BeSt: four treat-to-target strategies (sequential mono, step-up combo, initial combo + prednisone, initial infliximab + MTX), titrated to DAS44 ≤2.4.
JIP assignment: Patients were projected into the pre-existing four-cluster model (using the POODLE tool) from baseline clinical variables — age, sex, RF, ACPA, joint location (66/68 swollen + tender), ESR/CRP. Successfully classified 804/812 (99%) of NORD-STAR and 446/508 (88%) of BeSt.
Outcome — a deliberate methodological choice: Primary outcome was CDAI through week 48. CDAI was chosen specifically because it excludes acute-phase reactants (ESR/CRP) — which matters because tocilizumab artificially suppresses CRP/ESR, which would distort any index that includes them. Secondary: DAS28-CRP, HAQ, CDAI remission, CDAI50 (≥50% improvement), and (in BeSt) DAS44 and MTX-monotherapy retention.
Statistics: Mixed-effects models with each JIP subgroup tested against the other three combined, adjusted for baseline CDAI, time, and random effects for patient and treatment arm/strategy. Effects were then re-tested after adding age, sex, RF, ACPA, and symptom duration as covariates. A prespecified JIP × biologic-treatment interaction term tested whether csDMARDs vs bDMARDs behaved differently across subgroups.
The four subgroups (baseline profile):
- JIP-Foot: younger, foot small-joint dominant.
- JIP-Oligo: few involved joints, lowest activity.
- JIP-Hand: older, hand-dominant (note: hand-only polyarthritis was classified here), lower CDAI than Poly.
- JIP-Poly: highest disease activity — widespread hand + foot + large joints (median CDAI 38, TJC 28, SJC 17).
Notable serology gradient across groups: ACPA positivity fell from 83–84% (Foot/Oligo) to 66–68% (Hand/Poly) — i.e., the hand and poly groups were less seropositive, not more.
The Results
Primary outcome (CDAI):
- JIP-Hand → better response: Beta −1.4 (95% CI −2.3 to −0.55; p=0.0016) — i.e., ~1.4 CDAI points lower (better) than the other three groups, averaged across time.
- JIP-Poly → worse response: Beta +0.95 (95% CI 0.064–1.8; p=0.035).
- JIP-Foot and JIP-Oligo: no significant effect.
- Model fit was good (conditional R² ≈ 0.66–0.67).
- The JIP-Hand effect was directionally consistent in both trials, numerically larger in BeSt (−1.7) than NORD-STAR (−1.2) — plausibly because BeSt’s less aggressive older regimens let subgroup differences show through more.
Secondary outcomes reinforced JIP-Hand:
- Better DAS28-CRP (Beta −0.18, p=0.0028).
- Higher odds of CDAI remission (OR 1.7, 1.2–2.4).
- Higher odds of CDAI50 (OR 1.6, 1.1–2.2).
- No difference in HAQ (function) — Beta ≈ 0, p=0.86.
- CDAI- and DAS44-based analyses correlated tightly (r=0.95), arguing the effect is not just an artefact of 28-joint indices ignoring the feet.
JIP vs conventional predictors — the striking comparison:
- Female sex was the strongest conventional predictor of worse CDAI (Beta +1.2, p=0.0031).
- ACPA had NO significant effect on disease-activity response (Beta 0.19, p=0.67) — nor did RF.
- JIP-Hand remained independently protective even after adjusting for age, sex, RF, ACPA, and symptom duration (Beta −1.3, p=0.0039); JIP-Poly remained independently unfavourable. So the JIP effect is not just re-expressing sex or serology.
csDMARD vs bDMARD — no heterogeneity:
- The JIP × biologic interaction was non-significant for every subgroup (Hand p=0.58, Poly p=0.94, etc.).
- Translation: csDMARDs and bDMARDs were similarly effective (or ineffective) within each JIP subgroup. Adding a biologic did not selectively rescue the poor-prognosis Poly group.
MTX-monotherapy retention (BeSt treat-to-target):
- JIP-Hand trended toward higher retention on MTX monotherapy at week 24 (OR 1.5, 0.95–2.4, p=0.08) — consistent with the idea that hand-pattern patients respond adequately to standard MTX and need less escalation.
Clinical-relevance framing: Using published CDAI MCID thresholds (low-activity MCID = 1), the ~1.4-point JIP-Hand advantage clears the bar for low-disease-activity patients — modest but real. Overall, 77% (NORD-STAR) and 53% (BeSt) reached low activity/remission during follow-up.
Study Limitations
- Post hoc, non-randomised by JIP. Treatment wasn’t randomised within JIP subgroups (though randomisation was roughly balanced across them).
- Modest effect sizes. A 1.4-CDAI-point average difference is small; the authors repeatedly caution against over-reading it. This is risk refinement, not a treatment-selection rule.
- Partial circularity risk. JIP is derived from joint counts, and CDAI contains joint counts — so despite baseline-CDAI adjustment, residual confounding can’t be fully excluded. (They mitigate this with DAS44 replication.)
- Requires baseline joint mapping — limits point-of-care applicability, and subgroups sit on a continuum, so border cases get forced into one label.
- Underpowered for drug-specific effects. Only csDMARD-vs-bDMARD (lumped) was tested; specific-agent × JIP interactions may have been missed.
- ACPA analysed as positive/negative only (no titres); foot exams are noisier than hand exams, which may attenuate subgroup contrasts.
- Mechanism unknown — why hand-pattern does better and poly worse is unexplained (a synovial pathotype hypothesis is raised but untested here).
How This Study Adds to Practice
- Provides independent, cross-trial replication that a simple, routinely obtainable feature — where the arthritis is distributed — carries prognostic signal comparable to or larger than classical predictors.
- Delivers a provocative reframing: for short-term disease-activity response, joint distribution and sex outperform ACPA/RF, which are really radiographic-damage markers, not activity-response markers. A useful teaching correction to the reflex “seropositive = worse everything.”
- Suggests JIP-Poly patients are under-served by current strategies — and, importantly, that simply adding a biologic upfront does not preferentially fix them — flagging them as a target for future stratified trial designs.
- Positions JIP as an adjunct to existing prognostic factors for risk stratification and monitoring intensity, explicitly not (yet) a reason to change first-line therapy.
Final Takeaways
- In early RA, hand-dominant disease (JIP-Hand) predicts better treatment response (CDAI −1.4; remission OR 1.7; CDAI50 OR 1.6), while polyarthritis (JIP-Poly) predicts worse — independent of baseline activity, sex, and serology.
- The effect held across csDMARDs and bDMARDs with no interaction — early biologics did not selectively benefit any subgroup, including the poor-prognosis one.
- Sex beat serology: female sex was the strongest conventional predictor of higher disease activity; ACPA and RF showed no significant association with disease-activity response — a key conceptual point (they predict damage, not short-term activity).
- JIP-Hand patients were more likely to stay on MTX monotherapy — clinically, the group most likely to do well on standard first-line treatment.
- Effects are modest and hypothesis-generating. JIP subgrouping is a risk-stratification adjunct pending prospective validation, not a treatment-selection tool — and the biology behind the patterns remains unexplained (possibly distinct synovial pathotypes).