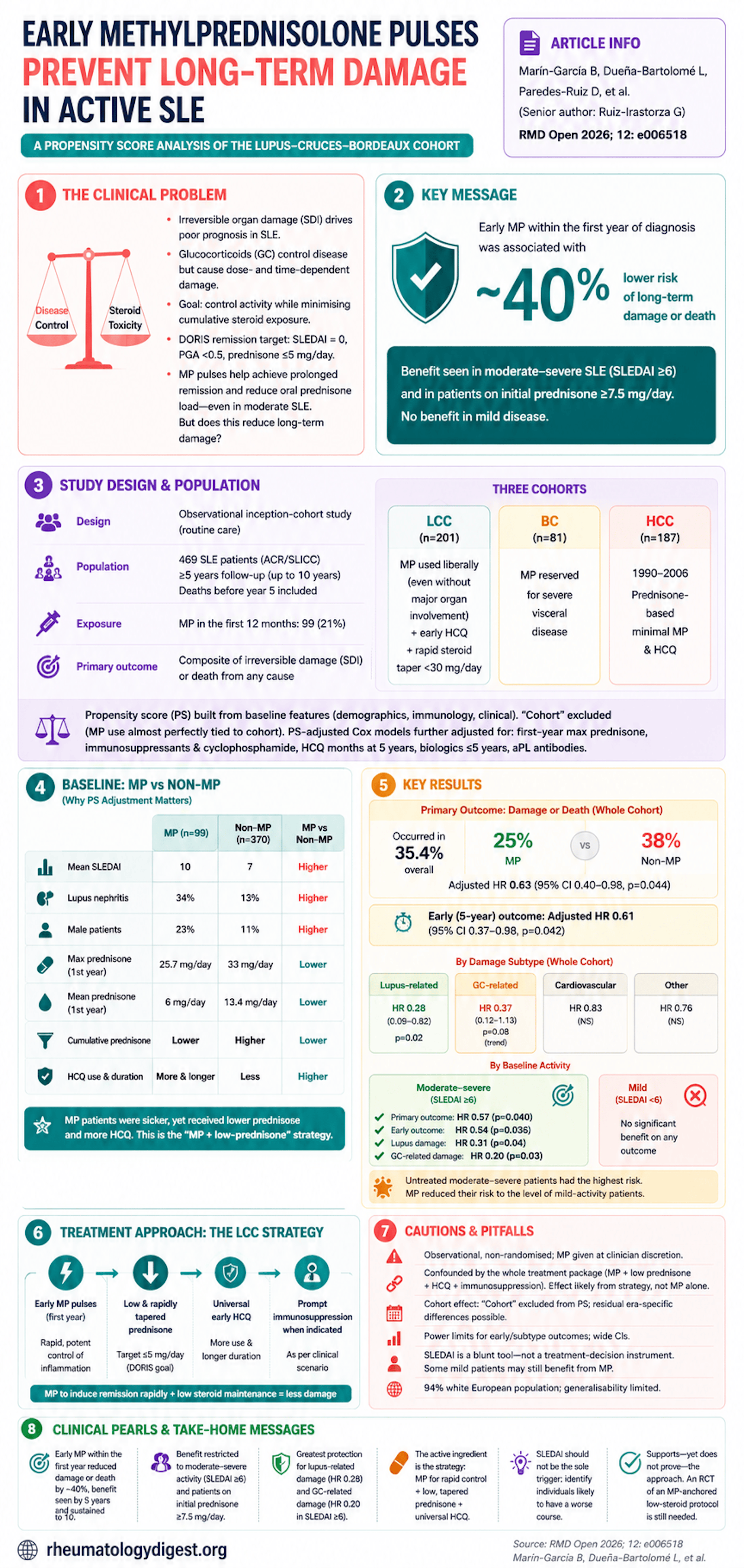
TL;DR: In this propensity-score–adjusted inception-cohort study, early (first-year) methylprednisolone pulses were associated with a ~40% reduction in long-term irreversible damage or death in active SLE — but only in moderate–severe disease, and the likely active ingredient is the strategy (MP to induce remission fast, paired with low, swiftly tapered oral prednisone and universal HCQ) rather than the molecule alone.
The Clinical Problem
In SLE, irreversible organ damage (measured by the SLICC Damage Index, SDI) is a central driver of poor prognosis — and there is a long-standing tension at the heart of treatment:
- Better disease control often requires glucocorticoids (GC).
- But GC themselves cause damage in a dose- and time-dependent way.
So the goal is to control activity while minimising cumulative steroid exposure. The DORIS remission target captures both objectives (clinical SLEDAI = 0, PGA <0.5, and prednisone ≤5 mg/day), and the 2023 EULAR guidelines have adopted it.
This group (Lupus–Cruces–Bordeaux) has previously shown that methylprednisolone pulses (MP) — rapid, potent, partly non-genomic anti-inflammatory bursts — help achieve prolonged remission and reduce oral prednisone load, even in moderate (not just severe) lupus. The unanswered question: does that translate into less long-term damage?
The Research Question
Does giving MP within the first year after SLE diagnosis reduce long-term irreversible damage accrual or death, and which patients benefit most?
The conceptual hypothesis is elegant: MP achieves faster and “better” remission while permitting lower oral prednisone, so it should reduce both lupus-driven and GC-driven damage that otherwise surfaces years later.
How the Study Was Designed
Design: Observational study using routine-care data from a longitudinal inception cohort (patients enrolled at diagnosis).
Population: 469 SLE patients (ACR and/or SLICC criteria) pooled from three sources:
- Lupus Cruces cohort (LCC, n=201) — where MP is used liberally, even without major organ involvement, followed by strict, rapidly tapered prednisone always <30 mg/day, universal HCQ.
- Bordeaux cohort (BC, n=81) — MP reserved for severe visceral disease.
- Historic Cruces cohort (HCC, n=187, diagnosed 1990–2006) — prednisone-based, minimal MP/HCQ use.
Follow-up: ≥5 years, up to 10 years. Patients who died before year 5 were deliberately included to avoid survivorship bias.
Exposure: MP given in the first 12 months (yes/no). 99 patients (21%) received MP.
Primary outcome: a composite of irreversible damage OR death from any cause over the whole follow-up (composite chosen specifically to defuse survivorship bias). Early outcome: the same composite at 5 years. Damage was further split into lupus-related, GC-related, cardiovascular, and “other” SDI subcategories.
Statistics — the key methodological point:
- A propensity score (PS) for receiving MP was built from demographic, immunological, and clinical baseline features.
- “Cohort” was deliberately left out of the PS because MP use was almost perfectly tied to which cohort a patient came from (LCC = MP, HCC = no MP); including it would have absorbed the very effect being studied.
- PS-adjusted Cox proportional-hazards models were then further adjusted for first-year max prednisone dose, first-year immunosuppressants and cyclophosphamide, cumulative HCQ months at 5 years, biologics within 5 years, and antiphospholipid antibodies.
- Analyses were run in the whole cohort and stratified by baseline activity: mild (SLEDAI <6) vs moderate–severe (SLEDAI ≥6).
Important baseline imbalance (why PS matters): MP-treated patients were sicker at baseline — higher SLEDAI (mean 10 vs 7), more nephritis (34% vs 13%), more men (23% vs 11%). Yet they received lower max and mean first-year prednisone (25.7 vs 33 mg/day; 6 vs 13.4 mg/day) and lower cumulative prednisone, plus more and longer HCQ. This is the “MP-plus-low-prednisone” strategy in action.
The Results
Remission (replicating prior work):
- 40.9% achieved prolonged DORIS remission; MP predicted it (PS-adjusted OR 1.97, 95% CI 1.12–3.46, p=0.017).
- Effect was confined to moderate–severe activity (OR 2.53, p=0.003); no effect in mild activity (OR 0.70, p=0.43).
- Prolonged remission itself was strongly protective against damage/death (HR 0.40, p<0.001).
Primary outcome (damage or death) — whole cohort:
- Occurred in 35.4% overall (25% of MP vs 38% of non-MP).
- Unadjusted KM curves showed only a trend (log-rank p=0.09) — but after PS adjustment, MP was significantly protective:
- Primary outcome: adjusted HR 0.63 (95% CI 0.40–0.98, p=0.044)
- Early (5-year) outcome: adjusted HR 0.61 (95% CI 0.37–0.98, p=0.042)
- That is roughly a ~40% relative reduction in damage/death, already evident by 5 years and sustained.
By damage subtype (whole cohort): the benefit was concentrated where the mechanism predicts:
- Lupus-related damage: adjusted HR 0.28 (0.09–0.82, p=0.02) — significant.
- GC-related damage: adjusted HR 0.37 (0.12–1.13, p=0.08) — strong trend.
- Cardiovascular and “other” damage: no significant effect (HR ~0.83 and ~0.76, NS).
Stratified by baseline activity — the central finding:
- Moderate–severe (SLEDAI ≥6): MP significantly protective — primary HR 0.57 (p=0.040), early HR 0.54 (p=0.036). For subtypes: lupus damage HR 0.31 (p=0.04); GC-related damage HR 0.20 (p=0.03).
- Mild (SLEDAI <6): no significant benefit on any outcome.
- Visually striking: untreated moderate–severe patients had the highest damage risk, but MP pulled their risk down to roughly the level of mild-activity patients.
Sensitivity analyses (robustness):
- Excluding the historic HCC cohort (analysing only LCC+BC, n=282): MP still protective for the primary outcome (HR 0.46, 0.22–0.97, p=0.043), though the early outcome lost significance (HR 0.56, p=0.16).
- Restricting to patients on initial prednisone ≥7.5 mg/day (above the toxicity threshold, n=292): MP protective for both primary (HR 0.59, p=0.035) and early (HR 0.58, p=0.044) outcomes.
Study Limitations
- Observational, non-randomised — MP was given at clinician discretion without a uniform protocol across cohorts; causation cannot be proven.
- Confounded by the whole treatment package. The MP signal is inseparable from the LCC strategy — MP plus rapid prednisone tapering plus universal early HCQ plus prompt immunosuppression. The authors candidly acknowledge that reduced cumulative GC load (not MP alone) likely contributes to the benefit. The honest message is arguably “the MP-anchored low-steroid protocol works,” more than “MP in isolation works.”
- Cohort effect. Because MP use and cohort were almost collinear, “cohort” couldn’t enter the PS; residual confounding from era-specific management (the older HCC) remains possible — though excluding HCC didn’t overturn results.
- Power limits for early/subtype outcomes — few early events widened CIs (e.g., GC-related and lupus early-damage trends were non-significant).
- SLEDAI as a blunt stratifier. Some “SLEDAI ≥6” patients (serologically active but clinically mild) received only HCQ or nothing; the authors stress SLEDAI is a research tool, not a treatment-decision instrument — and note some mild patients might still benefit from MP.
- Largely white European population (94%), limiting generalisability.
How This Study Adds to Practice
- It extends the rationale for MP beyond severe/organ-threatening lupus to moderate–severe activity, reframing MP as a first-choice remission-induction tool rather than a rescue-only therapy.
- It reinforces the “MP + reduced oral prednisone” paradigm now echoed in EULAR 2023: use a short potent burst to gain control, then keep maintenance prednisone low (ideally ≤5 mg/day) to spare long-term toxicity.
- It directly addresses the field’s biggest counter-argument — that MP simply adds steroid burden. Prior data (e.g., Sobhy et al.) linking high cumulative MP to harm were confounded by accompanying high oral prednisone; here, when MP is followed by low prednisone, GC-related damage is prevented, not increased.
- Practically, MP is cheap, widely available, and familiar — an accessibility argument the authors lean on for broader adoption.
Final Takeaways
- In this PS-adjusted inception-cohort study, early (first-year) MP was associated with a ~40% reduction in long-term damage or death (HR 0.63), visible by 5 years and sustained to 10.
- The benefit was restricted to moderate–severe baseline activity (SLEDAI ≥6) and to patients on initial prednisone ≥7.5 mg/day — and was absent in mild disease.
- The protection was mechanistically coherent: greatest for lupus-related (HR 0.28) and GC-related (HR 0.20 in the ≥6 subgroup) damage; no clear cardiovascular benefit.
- The likely active ingredient is the strategy, not the molecule alone — MP to induce remission rapidly, paired with low, swiftly tapered oral prednisone and universal HCQ.
- Caveat for interpretation: observational design plus cohort-linked confounding means this supports — rather than proves — the approach; an RCT of an MP-anchored low-steroid protocol remains the missing piece.
- Clinically: SLEDAI shouldn’t be the sole trigger for MP; the real task is identifying the individual destined for a worse course who stands to gain most.