TL;DR: On SIJ MRI, bone marrow oedema is the most sensitive but least specific sign of sacroiliitis — erosion is the key discriminator, lesion combinations and topographic location raise specificity, and semi-axial imaging plus clinical context are essential to avoid false-positive reads that can wrongly commit a patient to lifelong biologic therapy.
The Clinical Problem
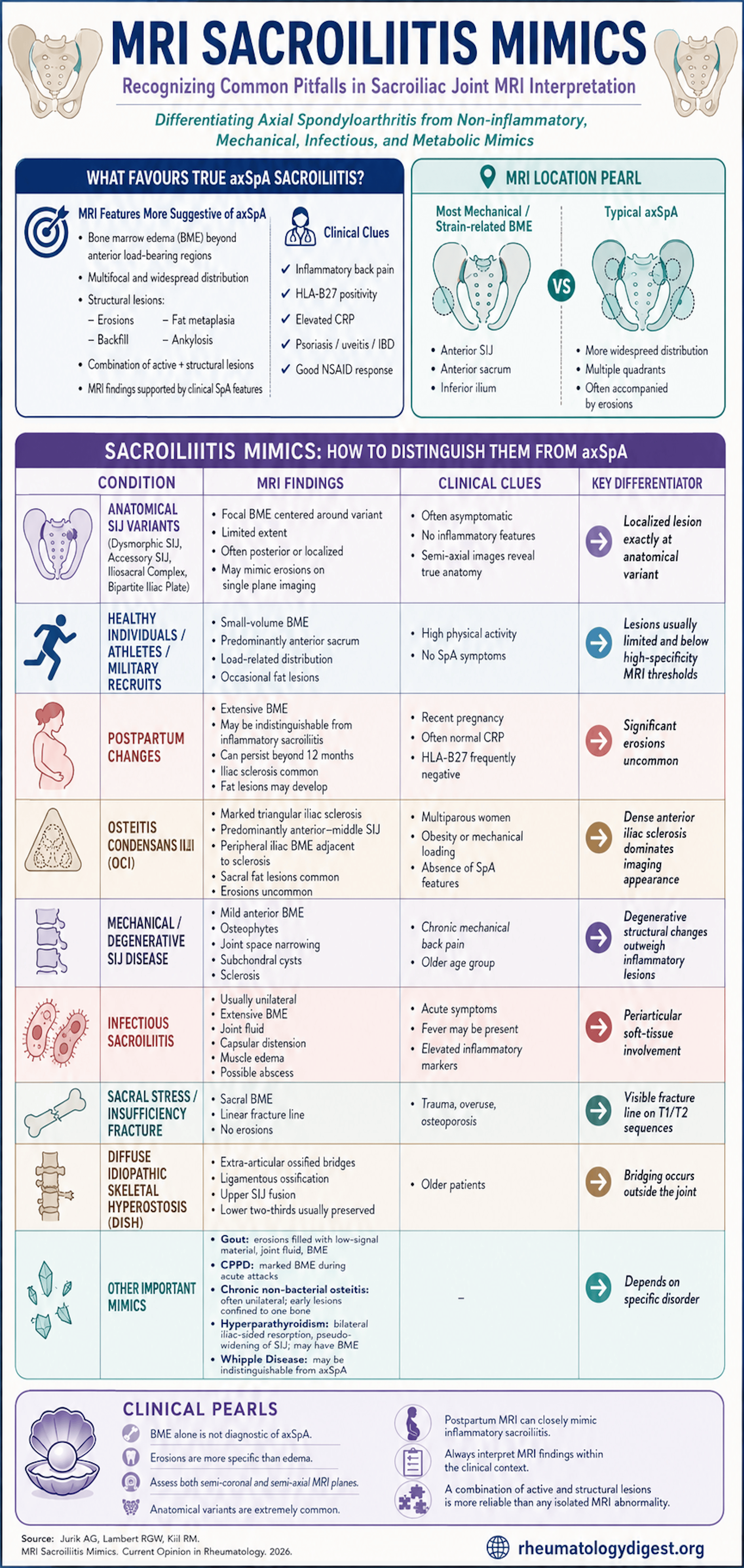
SIJ MRI is the imaging cornerstone for early axSpA, and subchondral bone marrow oedema (BME) is the most sensitive sign of active sacroiliitis — but it is among the least specific. BME appears in healthy people and in load-related, degenerative, traumatic, infectious, metabolic and other inflammatory conditions. Because an MRI labelled “sacroiliitis” can commit a patient to lifelong biologic therapy (or wrongly include them in a trial cohort), a false-positive read carries real consequences.
The review’s organising principle is a hierarchy of specificity:
- BME = sensitive, low specificity → the main source of overcalls.
- Structural lesions (erosion, sclerosis, fat metaplasia, backfill, ankylosis) = more specific; erosion is the key discriminator.
- Specificity rises further when lesions are combined and when their topographic location is taken into account.
Technique Is the First Defence Against Overcalling
The SIJ has two compartments — an anterior/inferior cartilaginous and a posterior/superior ligamentous part — with large interindividual (and even left-vs-right) variation. The single most important protocol point:
- Two perpendicular planes are mandatory — semi-coronal and semi-axial. Partial-volume effects on coronal-only imaging are a major source of pseudo-lesions.
- Recommended 4 sequences: STIR or T2-FS in both planes, a semi-coronal T1, and a cartilage-sensitive sequence (gradient echo or T1-FS).
- Hard data on why this matters: adding semi-axial images reduced the proportion of ASAS-positive healthy individuals by 33–56%, because much apparent “BME” in the lower posterior ilium was actually vascular signal, deep ligament insertions, or fluid-filled cysts.
Anatomical Variations — Common, and Commoner in Women
Present in 57–85% of non-axSpA individuals, up to 91% of healthy women vs 37% of men. Seven variations are described and can coexist. Only dysmorphic SIJ and unfused nuclei sit in the cartilaginous compartment; the rest are ligamentous-compartment variants that alter joint load and secondarily produce cartilaginous-compartment BME.
- Dysmorphic SIJ: facet prominence + opposing groove; focal, limited BME centred on the morphological change.
- Accessory SIJ: extra posterior joint; BME/sclerosis/fat can mimic sacroiliitis on semi-coronal — true location revealed on semi-axial.
- Iliosacral complex: iliac prominence + sacral groove with no osseous contact (so no adjacent BME), but vessels in the narrowed space can mimic enthesitis.
- Bipartite iliac bony plate: posterior iliac cleft; a vessel-filled channel that mimics BME and/or erosion.
- Lumbosacral transitional vertebrae: asymmetry shifts strain → BME.
Pearl: women carry a double risk — they have the highest rate of anatomical variants and are the group exposed to pregnancy-related and OCI changes.
“Background Noise” in Healthy People and Athletes
- ASAS-positive BME in 11.6–23.4% of healthy individuals <50 yrs; but BME exceeding the ≥95%-specificity data-driven threshold in only 2.5%.
- Athletes/military recruits: 4.3–41% meet ASAS criteria (more pronounced strain BME).
- Erosions reported in 0–20% and fat lesions in 4–20% of healthy/athletic individuals; lesions exceeding the 95% axSpA threshold were rare (fat thresholds crossed in 2–7%).
- Topographic rule: strain-related BME clusters at the anterior sacrum (and superior sacrum/inferior ilium on coronal), whereas axSpA is more widespread.
The Data-Driven ≥95% Specificity Cut-Offs
These thresholds are the practical tool for separating axSpA from most mimics:
- ASAS cut-offs: BME in ≥4 quadrants (or at the same location on ≥2 consecutive slices); erosions in ≥3 quadrants (or ≥2 consecutive slices); fat in ≥5 quadrants, on ≥3 consecutive slices, or >1 cm deep in ≥1 quadrant.
- Leiden cut-offs: ≥3 erosions, ≥3 fat lesions, or ≥5 erosions and/or fat lesions (each on ≥2 consecutive slices).
- Scored per the SPARCC system (BME on 6 semi-coronal STIR slices = 48 quadrants/patient; structural on 5 T1 slices = 40 quadrants/patient).
- Important caveat: these thresholds reliably separate axSpA from most mimics except OCI and postpartum change — the two hardest.
Pregnancy and Postpartum — the Toughest Mimic
- BME can appear at any stage of pregnancy and is frequent postpartum, with or without pain.
- A longitudinal study (103 first-time mothers) found BME peaks at 3 months postpartum. At 12 months, 41% still met ASAS criteria and 21% exceeded the ≥95% threshold.
- Depth and intensity can be as pronounced as axSpA — sometimes impossible to distinguish even at 12 months.
- What saves you: significant erosion is rare (though erosion-like lesions reported in up to 19%). Over time, BME converts to fat/sclerosis; iliac sclerosis ≥5 mm in 46% and ≥8 mm in 14% at 12 months — i.e. evolution toward OCI.
- Persistence is real but benign: ~16–17% still meet ASAS criteria at 2–5 years postpartum, yet axSpA-defining structural lesions do not develop — so structural change remains the long-term discriminator.
Osteitis Condensans Ilii (OCI)
- Manifest anterior iliac subchondral sclerosis in the middle third (weight-bearing), depth 11–13 mm, continuous from the articular surface.
- Predominantly parous women; also obesity/excess load (occasionally men, nulliparae).
- Concomitant BME in 48–93%, anterior-predominant. Distinguishing feature: iliac BME sits peripheral to the sclerosis as a thin continuous bright rim, unlike the subchondral, widespread iliac BME of true sacroiliitis.
- Erosions rare; sacral fat lesions frequent. Clinical context (childbirth, HLA-B27, CRP, absence of axSpA features) is essential.
Chronic Low Back Pain and Degeneration
- In 1037 chronic-LBP patients aged 18–40, ASAS-BME was present in 21.4% (fat 14.5%, sclerosis 8%, erosions 7.7%) — yet only 2.4% had axSpA at 3.5-year follow-up.
- Deep BME was not seen in non-axSpA LBP, and threshold-exceeding erosions/fat were rare. Again, anterior/load-related distribution vs widespread axSpA.
- Degenerative SIJ change is far commoner than axSpA and can appear in the 20s; osteophytes are poorly seen on MRI — only 55% of those on synthetic CT were visible on MRI, so cartilage-interface or sCT-like sequences help.
Less Common but Clinically Important Mimics
- DISH: extra-articular ossified bridges, partial fusion of the upper SIJ; lower two-thirds spared; erosions rare.
- Infectious sacroiliitis: usually unilateral, extensive BME with sacral predominance (not iliac-predominant), joint fluid, capsulitis, peri-articular/muscle oedema ± abscess — axSpA stays confined to bone and joint.
- Sacral fractures: BME most intense around fracture lines (black lines on T1/T2), no erosions.
- Others: Whipple’s (can be indistinguishable from axSpA), gout (intra-articular tophus material, erosions, BME), CPPD (profound BME in acute attacks), CNO (unilateral, single-bone early, lesions elsewhere), hyperparathyroidism (bilateral symmetric iliac subchondral resorption → pseudo-widening, no ankylosis or sacral erosions).
Key Takeaways
- BME alone never makes the diagnosis. It is the most sensitive but least specific finding; erosion is the most useful single discriminator, and lesion combinations (BME + erosion + fat) outperform any single lesion.
- Location, location, location. Strain-related/mechanical BME concentrates anteriorly; axSpA is widespread. The topographic check is the highest-yield habit.
- Always read semi-axial with semi-coronal — adding the axial plane cuts false-positives by one-third to one-half by exposing vascular/ligamentous pseudo-BME.
- Apply the ≥95%-specificity cut-offs, but know their blind spots: they do not reliably separate OCI or postpartum change from axSpA.
- Postpartum women and young athletes are the classic traps — BME can look identical to sacroiliitis, but the absence of evolving structural lesions over time (even up to 5 years) keeps them benign.
- Use clinical context as a sequence in its own right: parity, HLA-B27, CRP, symptom acuity, and unilaterality reshape the differential — especially toward infection, fracture, or metabolic disease when extensive erosion is present.