TL;DR: SLE management is organ- and severity-directed: the same drug list is deployed differently across nephritis, cutaneous, serositis and cytopenias, and because most effective agents suppress immune pathways — leaving infection a leading cause of mortality — the review foregrounds low-infection-risk metabolic and non-pharmacological strategies alongside the approved and off-label drugs.
Scope note: this summary covers FDA-approved SLE drugs and the off-label/used-in-practice agents anchored to the ACR 2025 SLE and 2024 lupus nephritis guidelines. Emerging/pipeline agents (CAR-T, BiTEs, CD40L, anti-CD38, TLR7/8 antagonists, atacicept/telitacicept, etc.) are excluded here and could be a separate summary.
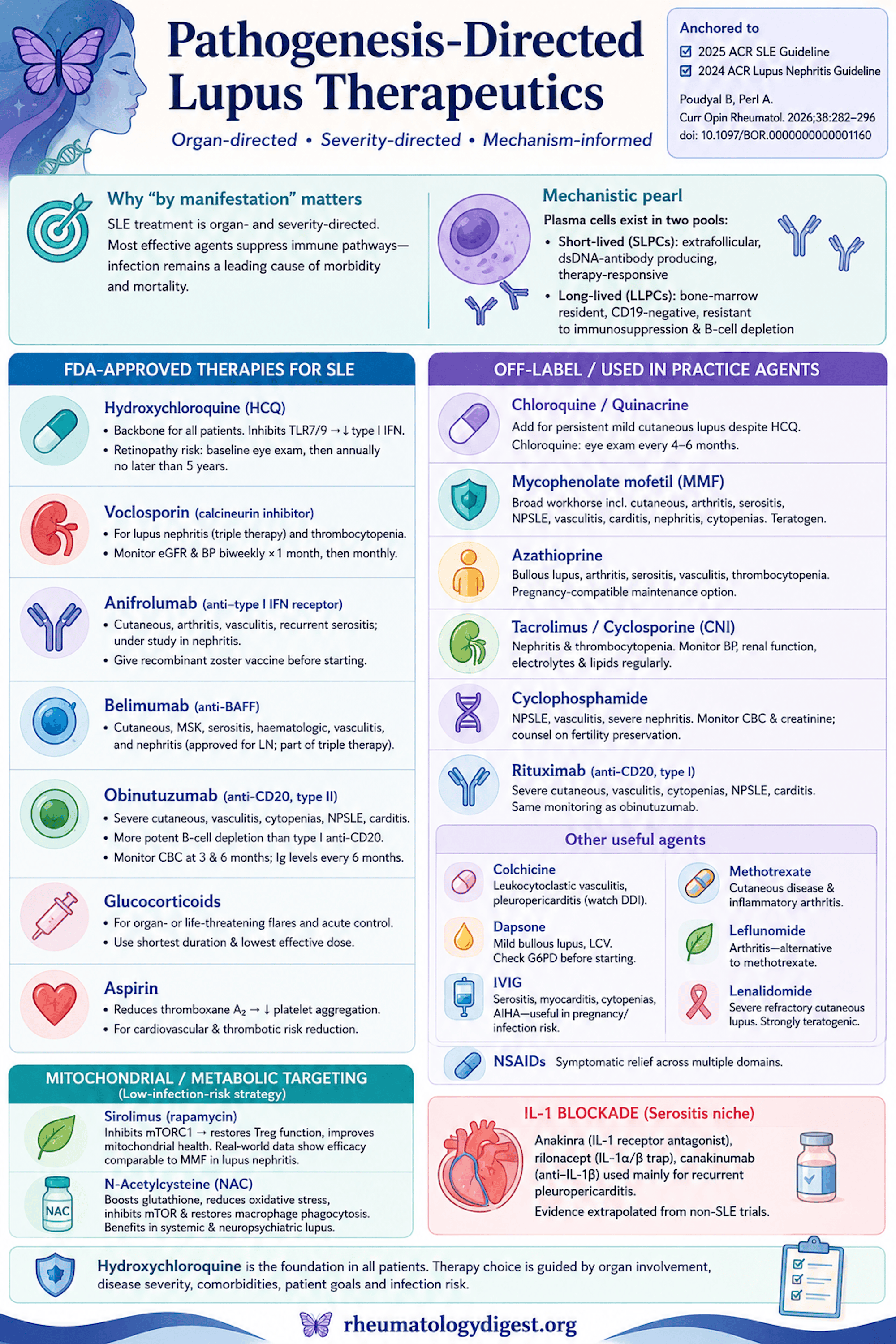
Framing: Why “By Manifestation” Matters
Contemporary SLE management is organ-directed and severity-directed, not one-size-fits-all. The same drug list gets deployed differently for nephritis vs cutaneous vs serositis vs cytopenias. A recurring trade-off runs through everything below: most effective agents suppress immune pathways, so infection remains a leading cause of morbidity/mortality — which is why the authors also foreground low-infection-risk options (diet, antioxidants, metabolic drugs).
One mechanistic pearl to hold onto: plasma cells split into short-lived plasma cells (SLPCs) — extrafollicular, dsDNA-antibody-producing, therapy-responsive — and long-lived plasma cells (LLPCs) — bone-marrow-resident, CD19-negative, and resistant to immunosuppression and B-cell depletion. This is the deep reason anti-CD20 and BAFF blockade often fail to deliver durable, drug-free remission.
FDA-Approved Therapies for SLE
Hydroxychloroquine (HCQ) — the backbone. Accumulates in lysosomes and raises pH, blocking autoantigen presentation, and inhibits TLR7/TLR9 signalling (less type I IFN and inflammatory cytokine production). Recommended for ALL patients with SLE unless contraindicated. Monitor CBC, renal/liver function, EKG if indicated. Retinopathy risk → ophthalmology screening (visual fields + OCT) at baseline, then annually no later than 5 years of use.
Voclosporin (calcineurin inhibitor). Inhibits calcineurin → blocks NFAT → less IL-2 and proinflammatory cytokines. Lupus nephritis (a component of modern triple therapy) and thrombocytopenia. Monitor eGFR and BP biweekly for the first month, then monthly.
Anifrolumab (anti-type I IFN receptor / IFNAR). Blocks the type I interferon axis central to lupus. Cutaneous, arthritis, vasculitis, recurrent pleuropericarditis; under study for lupus nephritis. Extension data: well tolerated, lower glucocorticoid use and improved SLEDAI. Practical pearl: give the recombinant zoster vaccine before starting (plus routine vaccination).
Belimumab (anti-BAFF/BLyS). Interferes with B-cell differentiation into antibody-producing plasma cells. Cutaneous, musculoskeletal, serositis, haematologic, vasculitis, and nephritis — approved for LN on the BLISS-LN trial and part of triple therapy.
Obinutuzumab (type II anti-CD20). Deep B-cell depletion via direct cell death, ADCC, ADCP and CDC (more potent depletion than type I anti-CD20). Severe bullous cutaneous, vasculitis, haemolytic anaemia, thrombocytopenia, neuropsychiatric, carditis. For CD20 antibodies: monitor CBC at 3 and 6 months and immunoglobulin levels every 6 months.
Glucocorticoids. Bind the intracellular GC receptor → transactivate anti-inflammatory and suppress proinflammatory genes. Organ- or life-threatening flares and acute control — but at the shortest duration and lowest dose (cumulative steroid is a major driver of damage).
Aspirin. Acetylates COX-1 → less thromboxane A2 → less platelet aggregation. Cardiovascular and thrombotic risk reduction.
Off-Label / Approved-for-Other-Indications but Used in SLE
Chloroquine. Same antimalarial mechanism as HCQ. Role: mild ongoing cutaneous lupus despite HCQ. Retinopathy screening is more frequent — baseline then every 4–6 months.
Quinacrine. Added to HCQ for persistent mild cutaneous lupus despite topical therapy. Practical limits: availability only via compounding pharmacies and cost.
Mycophenolate mofetil (MMF). Prodrug → mycophenolic acid → inhibits IMPDH → less guanine nucleotide synthesis → reduced lymphocyte proliferation. Broad workhorse: moderate–severe cutaneous, arthritis, recurrent pleuropericarditis, neuropsychiatric, vasculitis, carditis, nephritis, thrombocytopenia. Teratogen — urine pregnancy testing at baseline, ~8–10 days, and follow-ups; CBC at baseline, 2 weeks, then regularly.
Azathioprine. Prodrug → 6-mercaptopurine → thioguanine nucleotides → inhibits DNA synthesis/proliferation. Bullous lupus, arthritis, recurrent pleuropericarditis, vasculitis, thrombocytopenia. A common pregnancy-compatible maintenance option.
Tacrolimus and cyclosporine (calcineurin inhibitors). Same NFAT/IL-2 mechanism as voclosporin. Nephritis and thrombocytopenia. Monitoring is heavier: CBC/LFT monthly ×3 then q3-monthly; lipids q6-monthly; creatinine/Mg/K every 2 weeks ×3 months then monthly; BP regularly.
Cyclophosphamide (alkylating agent). Hepatically activated → cross-links DNA. Use has declined as less toxic options arrived, but still relevant for neuropsychiatric lupus, vasculitis, and severe nephritis. Monitor CBC and creatinine weekly ×1 month then monthly; urinalysis with every infusion and 6-monthly afterward; urine pregnancy before each infusion; counsel on fertility preservation.
Rituximab (type I anti-CD20). B-cell depletion via ADCC/CDC, apoptosis, reduced proliferation. Severe bullous cutaneous, vasculitis, haemolytic anaemia, thrombocytopenia, neuropsychiatric, carditis. Same CD20 monitoring as obinutuzumab.
Colchicine. Inhibits microtubule polymerisation → impairs neutrophil activation/migration/degranulation. Leukocytoclastic vasculitis and pleuropericarditis. Pearl: CYP3A4 metabolism → watch for drug–drug interactions.
Dapsone. Reduces neutrophil superoxide/elastase and adhesion/chemotaxis. Mild bullous lupus and leukocytoclastic vasculitis. Check G6PD before starting; CBC/LFT weekly ×1 month, monthly ×3, then quarterly.
IVIG. Multimodal — Fc-receptor and FcRn blockade, reduced complement-mediated damage, B/T-cell regulation. Pleuropericarditis, myocarditis, thrombocytopenia, haemolytic anaemia (useful when infection or pregnancy limits immunosuppression). Monitor CBC monthly for haemolysis.
Methotrexate. Inhibits DHFR (plus adenosine release, NF-κB inhibition). Cutaneous disease and inflammatory arthritis. CBC/LFT/renal monthly ×3 then quarterly.
Leflunomide. Inhibits DHODH (pyrimidine synthesis); at higher doses affects T/B-cell tyrosine-kinase signalling. Arthritis — alternative to MTX. Same monitoring as MTX.
Lenalidomide. Cereblon modulator; suppresses proinflammatory cytokines. Reserved for severe refractory cutaneous lupus after other therapies fail. Strongly teratogenic — urine pregnancy test 24 h before initiation, weekly in month 1, then every 2–4 weeks.
NSAIDs. COX inhibition for symptomatic relief across multiple domains (use cautiously given renal/CV/GI risk).
At-a-Glance: Approved and Off-Label Drugs
| Drug | Class / mechanism | Main SLE use | Key monitoring |
|---|---|---|---|
| Hydroxychloroquine | Antimalarial; ↓TLR7/9, ↓type I IFN | All patients (backbone) | CBC, renal/liver, EKG; eye screen baseline + annually by 5 yrs |
| Voclosporin | Calcineurin inhibitor (↓NFAT/IL-2) | Lupus nephritis (triple therapy); thrombocytopenia | eGFR + BP biweekly ×1 mo, then monthly |
| Anifrolumab | Anti-IFNAR (type I IFN) | Cutaneous, arthritis, vasculitis, pleuropericarditis; LN under study | Give RZV before starting; routine vaccination |
| Belimumab | Anti-BAFF/BLyS | Cutaneous, MSK, serositis, haematologic, vasculitis, nephritis | Standard; infection vigilance |
| Obinutuzumab | Type II anti-CD20 (deep depletion) | Severe bullous, vasculitis, AIHA, thrombocytopenia, NPSLE, carditis | CBC at 3 & 6 mo; immunoglobulins q6-monthly |
| Rituximab | Type I anti-CD20 | As obinutuzumab (severe/refractory) | As CD20 above |
| Glucocorticoids | GC-receptor gene modulation | Organ/life-threatening flares, acute control | Shortest duration, lowest dose |
| Aspirin | COX-1 acetylation (↓TXA2) | CV / thrombotic risk reduction | — |
| Chloroquine | Antimalarial (as HCQ) | Mild cutaneous despite HCQ | Eye screen baseline then q4–6 mo |
| Quinacrine | Antimalarial | Persistent mild cutaneous (add-on) | Compounding-only; cost |
| Mycophenolate mofetil | ↓IMPDH (↓lymphocyte proliferation) | Broad workhorse incl. nephritis | Teratogen — pregnancy tests; CBC baseline, 2 wk, then regular |
| Azathioprine | Purine antimetabolite | Bullous, arthritis, serositis, vasculitis, thrombocytopenia | CBC/LFT; pregnancy-compatible maintenance |
| Tacrolimus / cyclosporine | Calcineurin inhibitors | Nephritis, thrombocytopenia | CBC/LFT, Cr/Mg/K, lipids, BP (heavy schedule) |
| Cyclophosphamide | Alkylating agent (DNA cross-link) | NPSLE, vasculitis, severe nephritis | CBC/Cr, urinalysis, pregnancy test; fertility counselling |
| Colchicine | ↓Microtubules (neutrophil) | Leukocytoclastic vasculitis, pleuropericarditis | CYP3A4 drug interactions |
| Dapsone | ↓Neutrophil superoxide/chemotaxis | Mild bullous, leukocytoclastic vasculitis | Check G6PD; CBC/LFT |
| IVIG | Fc/FcRn blockade, immunomodulation | Serositis, myocarditis, thrombocytopenia, AIHA | CBC monthly for haemolysis |
| Methotrexate | ↓DHFR (+ adenosine, ↓NF-κB) | Cutaneous, inflammatory arthritis | CBC/LFT/renal monthly ×3 then quarterly |
| Leflunomide | ↓DHODH (pyrimidine synthesis) | Arthritis (MTX alternative) | As MTX |
| Lenalidomide | Cereblon modulator | Refractory cutaneous | Strongly teratogenic — strict pregnancy testing |
| NSAIDs | COX inhibition | Symptomatic relief | Renal/CV/GI caution |
Mitochondrial / Metabolic-Targeting Agents (Low-Infection-Risk Strategy)
A distinctive theme of this review: lupus T cells are metabolically abnormal — mitochondrial hyperpolarisation, reduced ATP, increased ROS, glutathione depletion, and mTOR activation — which can be targeted without broad immunosuppression.
Sirolimus (rapamycin). Binds FKBP-12 → inhibits mTORC1 → shifts the T-cell balance away from TH1/TH17/TFH and restores Treg function; stabilises mitochondrial membrane potential and calcium flux. Renal and non-renal SLE. Evidence: a real-world CSTAR cohort showed efficacy comparable to MMF in lupus nephritis with improved complement; a 21-year follow-up showed durable clinical/serological benefit; and it reverses IL-21-driven Treg dysfunction.
N-acetylcysteine (NAC). Glutathione precursor → reverses oxidative stress, inhibits mTOR, and restores macrophage phagocytosis (notably countering anti-phosphatidylserine antibodies that impair immune-complex clearance). Studied benefit in systemic disease including neuropsychiatric and hepatic manifestations — attractive because it does not raise infection risk.
IL-1 Blockade (Serositis Niche)
Anakinra (IL-1 receptor antagonist), rilonacept (IL-1α/β trap) and canakinumab (anti-IL-1β) are used mainly for recurrent pleuropericarditis — though the evidence is largely indirect, extrapolated from non-SLE recurrent pericarditis trials.
Cardiometabolic Adjuncts (Comorbidity-Directed)
These are approved for diabetes/cardiometabolic disease and used/studied in SLE for organ protection rather than immunosuppression:
- Metformin — AMPK-dependent and -independent anti-inflammatory effects; potential benefit in nephritis and reduced cardiovascular events.
- SGLT2 inhibitors — possible renal/cardiovascular protection (reduced AKI, CKD, heart failure).
- GLP-1 receptor agonists — possible favourable cardiovascular/renal outcomes with putative immunomodulatory effects.
All are under active study and currently positioned as comorbidity-targeted adjuncts, not disease-modifying lupus therapy.
Non-Pharmacological Measures (Recommended, Infection-Neutral)
Photoprotection, smoking cessation, and exercise (aerobic + resistance) are guideline-supported. Mechanistically, gut dysbiosis drives tryptophan→kynurenine metabolism that activates mTOR in T cells; dietary tryptophan restriction reduced autoimmunity in murine models — an emerging rationale for diet as adjunct.
Quick Map by Manifestation
- Backbone (all patients): hydroxychloroquine.
- Lupus nephritis: MMF or cyclophosphamide ± belimumab and/or a calcineurin inhibitor/voclosporin (triple therapy); sirolimus as an emerging option.
- Cutaneous: topicals → HCQ → add quinacrine/chloroquine → MMF, methotrexate, anifrolumab/belimumab → dapsone (bullous) → lenalidomide (refractory).
- Inflammatory arthritis: methotrexate, leflunomide, belimumab.
- Serositis / recurrent pleuropericarditis: colchicine, NSAIDs, IL-1 blockers, azathioprine/MMF, IVIG.
- Haematologic (cytopenias, AIHA): glucocorticoids, rituximab/obinutuzumab, IVIG, MMF/azathioprine, calcineurin inhibitors.
- Neuropsychiatric: cyclophosphamide, MMF, rituximab/obinutuzumab; NAC as adjunct.
- Vasculitis: glucocorticoids, cyclophosphamide, rituximab/obinutuzumab, belimumab, anifrolumab; colchicine/dapsone for leukocytoclastic.
- Cardiovascular/thrombotic risk: aspirin, HCQ, and the cardiometabolic adjuncts.