TL;DR: SSc kidney disease is a spectrum, not just scleroderma renal crisis (SRC) — but when SRC is suspected, immediate ACE inhibition (captopril) is the single most important action, started before any confirmatory test and never stopped for a rising creatinine; despite this, prognosis has plateaued since ~2015.
The Clinical Problem
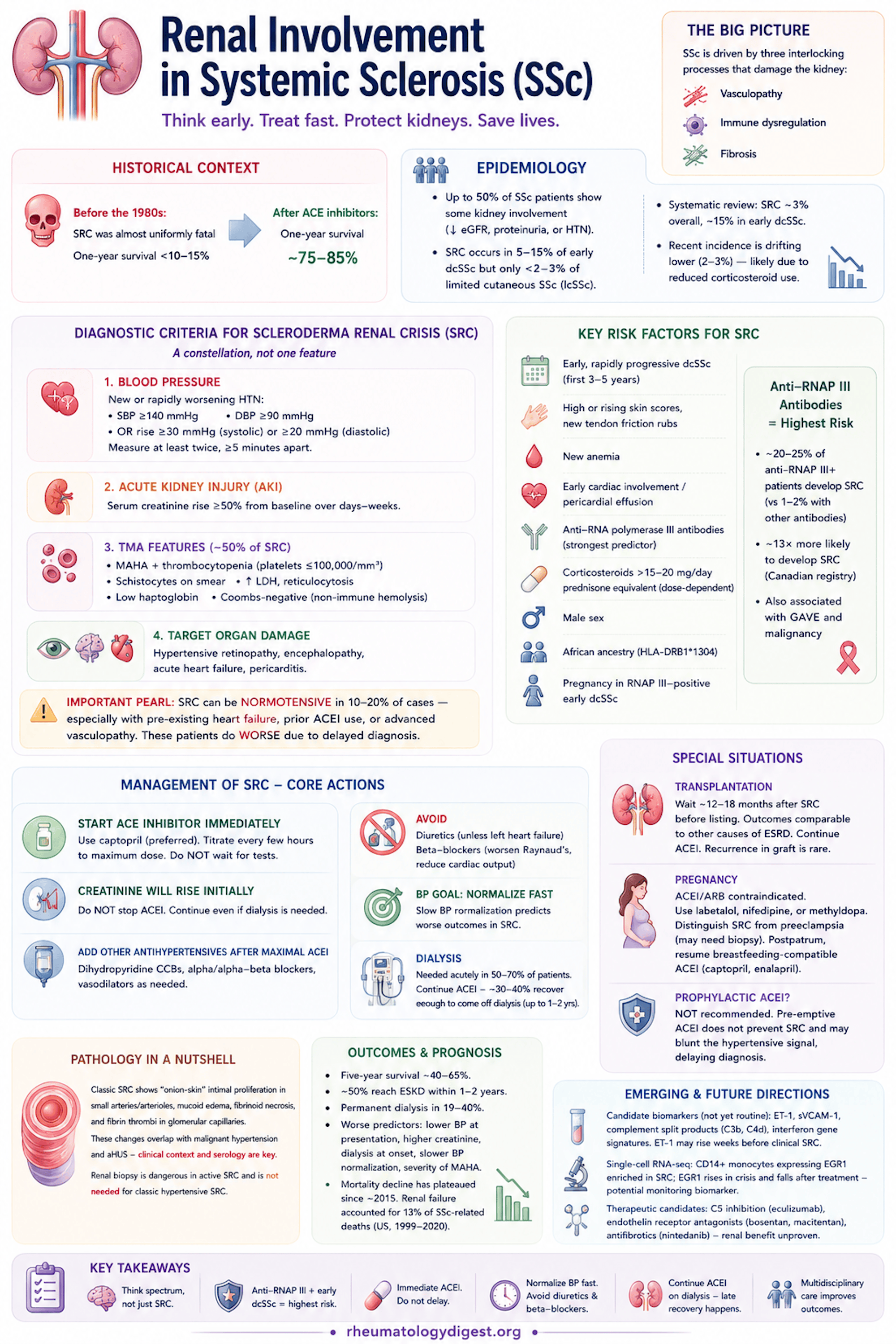
Systemic sclerosis (SSc) is an autoimmune connective tissue disease driven by three interlocking processes: vasculopathy, immune dysregulation, and fibrosis. The kidney is a key target organ, and renal disease is a major driver of morbidity and mortality, especially in early diffuse cutaneous SSc (dcSSc) with anti-RNA polymerase III (anti-RNAP III) positivity.
The most feared manifestation is scleroderma renal crisis (SRC) — an emergency of abrupt severe hypertension with rapidly progressive acute kidney injury (AKI), caused by arteriolar vascular injury. The historical context frames its importance:
- Before the 1980s, SRC was almost uniformly fatal — one-year survival under 10–15%.
- After the introduction of ACE inhibitors (ACEI), one-year survival rose to roughly 75–85%.
A crucial conceptual point the authors stress: renal disease in SSc is NOT synonymous with SRC. There is a broader spectrum — chronic vasculopathic nephropathy, proteinuria, thrombotic microangiopathy (TMA), normotensive SRC, overlap glomerulonephritides, and drug-induced injury — that collectively carries a higher overall burden than SRC alone.
Key Epidemiology
- Up to 50% of SSc patients show some kidney involvement (reduced eGFR, proteinuria, or hypertension).
- SRC occurs in 5–15% of dcSSc but only <2–3% of limited cutaneous SSc (lcSSc).
- A systematic review found SRC in ~3% overall, rising to ~15% in early dcSSc.
- Non-obvious point: the more recent SRC incidence figures are drifting lower (2–3%), partly attributed to reduced corticosteroid use — i.e., changing prescribing is reshaping the epidemiology.
Diagnostic Criteria for SRC — a Constellation, Not One Feature
- Blood pressure: new/rapidly worsening HTN — SBP ≥140, DBP ≥90, OR a rise of ≥30 (systolic)/≥20 (diastolic) from baseline. Measure at least twice, ≥5 min apart.
- AKI: serum creatinine rise ≥50% from baseline over days–weeks.
- TMA features: MAHA + thrombocytopenia (platelets ≤100,000), schistocytes, high LDH, low haptoglobin, Coombs-negative (supports non-immune hemolysis). About half of SRC patients show TMA.
- Target-organ damage: hypertensive retinopathy, encephalopathy, acute heart failure, pericarditis.
Critical teaching pearl: SRC can be normotensive (10–20% of cases) — especially with pre-existing heart failure, prior ACEI use, or advanced vasculopathy. These do worse because diagnosis is delayed. Do not let “normal BP” exclude SRC if creatinine is climbing in early dcSSc.
Pathophysiology — Five Converging Mechanisms
- Microvascular dysfunction: endothelial injury → reduced vasodilators (NO, prostacyclin), excess endothelin-1 (ET-1), upregulated adhesion molecules, prothrombotic state.
- RAAS activation: juxtaglomerular ischaemia → renin surge → vicious cycle of vasoconstriction and TMA. This is why ACEI work so well — and why ACEI are preferred over ARBs: ACEI raise bradykinin (an efferent-arteriole vasodilator), whereas ARBs do not, so ARBs are not used alone in SRC.
- Autoantibodies: anti-RNAP III is the strongest serologic predictor. ~20–25% of anti-RNAP III–positive patients develop SRC vs 1–2% of anti-topoisomerase I or anti-centromere patients. In a Canadian registry, SRC was ~13× more likely if RNAP III positive. Anti-Scl-70 and anti-centromere are not associated with SRC (centromere may even be protective). Anti-RNAP III also flags GAVE and a malignancy association — worsening skin shortly after a cancer diagnosis is a red flag.
- Fibrosis: TGF-β, PDGF, CTGF, interferon-regulated genes; single-cell work identifies a distinct kidney fibroblast subset (high COL1A1, PDGFRB, NOTCH) — a potential antifibrotic target.
- Complement & TMA: classical/lectin/alternative pathway activation; C4d deposition in peritubular capillaries; SRC may sit on a spectrum with atypical HUS (aHUS) — hence interest in C5 inhibition (eculizumab case reports).
Histology
- Pathognomonic concentric “onion-skin” intimal proliferation in small arteries/arterioles.
- Mucoid intimal oedema, fibrinoid necrosis, fibrin thrombi in glomerular capillaries, and (advanced) ischaemic glomerular collapse / cortical necrosis.
- Key caveat: these lesions overlap with malignant hypertension and aHUS — so clinical context + serology drive diagnosis, not histology alone.
- Renal biopsy is dangerous in active SRC (bleeding risk from severe HTN and impaired small-vessel contraction) and is not needed for classic hypertensive SRC.
Risk Factors
- Early rapidly progressive dcSSc (first 3–5 years), high/rising skin scores, new tendon friction rubs, new anaemia, early cardiac involvement / pericardial effusion.
- Corticosteroids: dose-dependent risk, especially >15–20 mg/day prednisone equivalent — though confounded by the fact that high-activity disease is both steroid-treated and inherently high-risk. Avoid steroids where possible in early dcSSc.
- Anti-RNAP III, male sex (proportionately more dcSSc/SRC), African ancestry (HLA-DRB1*1304), pregnancy in RNAP III–positive early dcSSc.
Management — the Core Actions
- Start ACEI immediately when SRC is suspected — do NOT wait for labs, imaging, or biopsy. Captopril is favoured for its short half-life and rapid titratability; titrate every few hours to maximum dose.
- Expect creatinine to rise initially — do NOT stop the ACEI for this. Continue ACEI even if dialysis is needed.
- Add other antihypertensives (dihydropyridine CCBs, alpha/alpha-beta blockers, vasodilators) only after maximal ACEI if BP remains high.
- Avoid diuretics unless there is left heart failure (volume is high but circulating volume is contracted by vasoconstriction). Avoid beta-blockers (worsen Raynaud’s, reduce cardiac output).
- Counter-intuitive BP goal: normalize BP quickly — unlike chronic malignant hypertension where rapid lowering risks brain hypoperfusion. Slow BP normalisation in SRC predicts worse outcomes.
- Dialysis: needed acutely in 50–70%; continue ACEI because ~30–40% recover enough to come off dialysis, sometimes up to 1–2 years later.
- Transplant: wait ~12–18 months after SRC before listing (allow late recovery); outcomes comparable to other ESRD causes; recurrence in the graft is rare; continue ACEI.
- PLEX: not routine; consider only in refractory severe TMA or overlap (e.g., anti-GBM).
Prophylactic ACEI — Explicitly NOT Recommended
Pre-emptive ACEI does not prevent SRC and may blunt the hypertensive signal, delaying diagnosis.
Pregnancy
ACEI/ARB contraindicated — use labetalol, nifedipine, or methyldopa. Distinguish SRC from preeclampsia (may need biopsy). Postpartum, resume breastfeeding-compatible ACEI (captopril, enalapril).
Outcomes / Prognosis
- Five-year survival remains modest at ~40–65% (driven by cardiac disease, ILD, progressive CKD).
- ~50% of SRC patients reach ESKD within 1–2 years; permanent dialysis in 19–40%.
- Worse-outcome predictors: lower BP at presentation, higher creatinine, dialysis at onset, slower BP normalisation, severity of MAHA.
- Sobering point: mortality decline has plateaued since ~2015 — no further improvement in the recent decade despite modern care. Renal failure accounted for 13% of SSc-related deaths (US, 1999–2020).
Precision Medicine / Emerging Directions
- Candidate biomarkers (not yet routine): plasma ET-1, soluble VCAM-1, complement split products (C3b, C4d), interferon gene signatures. ET-1 may rise weeks before clinical SRC.
- Single-cell RNA-seq: CD14+ monocytes expressing EGR1 enriched in SRC; EGR1 rises during crisis and falls after treatment — a possible monitoring biomarker.
- Therapeutic candidates: C5 inhibition, endothelin receptor antagonists (bosentan, macitentan), antifibrotics (nintedanib) — renal benefit currently unproven.
Key Takeaways
- Think of SSc kidney disease as a spectrum, not just SRC — chronic nephropathy, TMA, normotensive SRC, and overlaps all matter, and CKD is an independent mortality predictor.
- Anti-RNAP III + early dcSSc defines the highest-risk patient — these patients need close BP, creatinine, and urinalysis surveillance (consider home BP monitoring; creatinine/eGFR every 1–3 months in the first years).
- When SRC is suspected, immediate ACEI (captopril) is the single most important action — never delayed for confirmatory tests, and never stopped for a rising creatinine.
- Avoid high-dose steroids in early dcSSc; do not use prophylactic ACEI.
- Normalize BP fast; avoid diuretics and beta-blockers; biopsy is reserved for normotensive/atypical presentations or suspected overlap (ANCA, immune-complex GN).
- Continue ACEI on dialysis — late renal recovery is real (up to ~40%).
- Despite ACEI, prognosis has stalled — driving interest in complement-directed therapy, biomarkers, and multi-omics risk stratification, but none is yet ready for routine use.
- Multidisciplinary care (rheumatology + nephrology, plus cardiology/obstetrics) is essential.