TL;DR: A 2026 RMD Open narrative review concludes that the adjuvanted recombinant zoster vaccine (RZV) offers substantial protection in inflammatory rheumatic disease — ~95% reduction in HZ recurrence in real-world cohorts, 54–70% effectiveness in SLE — with no meaningful short-term flare signal in RCT data, shifting the clinical question from whether to vaccinate to how to ensure it actually happens.
The Clinical Problem
Herpes zoster (HZ) and postherpetic neuralgia (PHN) impose a heavy burden in older and immunocompromised adults. Several points frame the issue:
- Background HZ incidence in the general population is roughly 2–9 per 1000 person-years, and higher in the immunocompromised.
- Patients with inflammatory rheumatic disease (IRD) carry a 1.5–2 fold higher HZ risk than non-inflammatory controls, even after adjustment for age and comorbidities. Some subgroups — notably young patients with SLE — approach or exceed the risk seen in immunocompetent adults ≥50 years.
- Therapy is a strong risk modifier. High-dose glucocorticoids (GC), B-cell- and T-cell-directed bDMARDs, and especially JAK inhibitors consistently emerge as strong risk factors. Prior HZ, longer disease duration and concomitant GC use amplify risk further.
- The historical preventive gap: the live-attenuated zoster vaccine (ZVL) was contraindicated in most clinically relevant immunosuppression, could only be used in selected stable low-immunosuppression patients (typically pre-bDMARD), and showed only moderate efficacy (~50–70%) with sparse rheumatology safety data.
The non-live, adjuvanted recombinant zoster vaccine (RZV) was developed to close this gap — but its efficacy, durability, safety and (critically for rheumatologists) flare risk under active immunosuppression needed clarification.
Vaccine Composition and Immunologic Rationale
- RZV combines the VZV glycoprotein E (gE) antigen with the AS01B adjuvant (a liposomal system containing monophosphoryl lipid A and QS-21).
- It is non-replicating, hence safe to give under immunosuppression (general vaccination contraindications still apply).
- A clinically important concept: protection against VZV reactivation is driven mainly by VZV-specific CD4+ T-cell immunity, while circulating antibody titres correlate only imperfectly with clinical protection — particularly in older and immunosuppressed patients.
- A non-obvious implication: in immunocompromised cohorts, RZV induces robust CD4+ T-cell responses even when antibody titres are attenuated. Relying on serological endpoints alone may therefore underestimate true vaccine-induced protection in IRD.
- AS01-type adjuvants generate interferon-related innate immune signatures linked to immunogenicity — a double-edged point, relevant both to SLE (type I interferon-driven disease) and to JAK inhibitors (which pharmacologically blunt downstream IFN/cytokine signalling).
Efficacy in the General Adult Population
- ZOE-50: vaccine efficacy against HZ 97.2% in adults ≥50 years (median 3.1-year follow-up).
- ZOE-70: efficacy 89.8% in adults ≥70 years (median 3.7-year follow-up).
- Long-term (ZOE-LTFU): efficacy 81.6% during years 5.6–9.6 post-vaccination; cumulative efficacy 89.0% from 1 month after dose 2 through a mean of 9.6 years. Anti-gE antibodies persisted >5-fold above baseline and gE-specific CD4+ T cells >6-fold above baseline through year 10, with no new safety signals.
Take-home: in immunocompetent adults, two doses provide at least a decade of clinically meaningful protection.
Efficacy and Safety in Immunocompromised Populations
Based on RCTs and observational data, ACIP concluded RZV confers substantial benefit in immunocompromised adults ≥19 years:
- Efficacy against HZ ranged from ~68% (autologous haematopoietic cell transplant) to 85–90% (haematologic malignancies, potential immune-mediated diseases).
- Across 6 RCTs in immunocompromised cohorts: humoral response rates 65–96% and cell-mediated response rates 50–93% — far above placebo, though absolute titres/T-cell frequencies were somewhat lower than in immunocompetent adults.
- Serious adverse events and immune-mediated disease events occurred at similar rates in RZV and placebo arms.
Rheumatology-Specific Evidence
The review integrates three complementary evidence streams:
A) Aikawa et al — Brazilian phase 4 RCT (the most robust IRD-specific data)
Single-centre, double-blind, placebo-controlled non-inferiority trial; 1192 adults with IRD (RA, SLE, spondyloarthritis and others) on stable GC and/or DMARD therapy, randomised 1:1 to two RZV doses or placebo 6 weeks apart; an additional 393 healthy controls received open-label RZV.
- Primary endpoint: disease flare up to day 84 after the first dose. Non-inferiority declared if the upper one-sided 95% CI for the between-group flare difference was <5%.
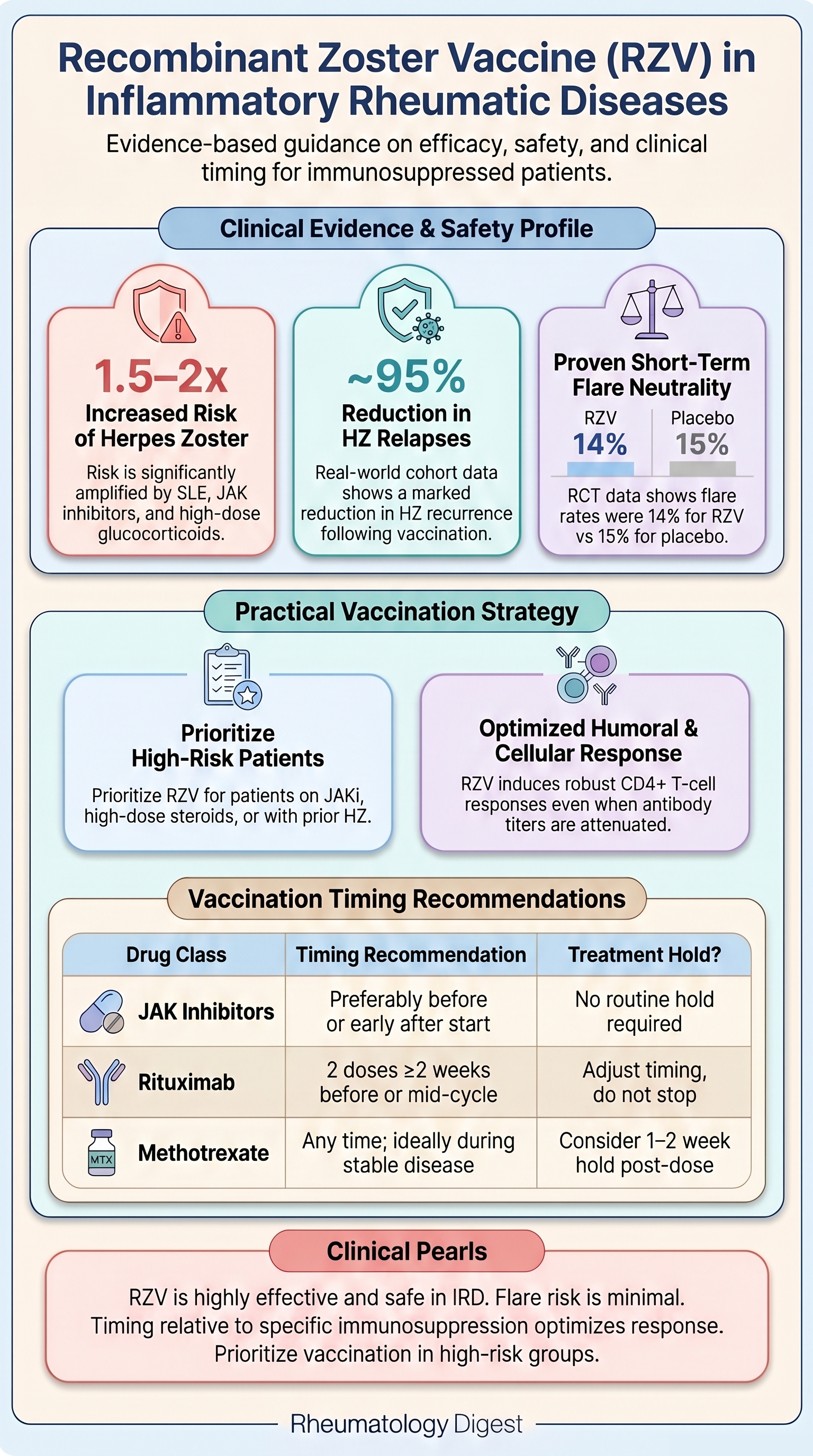
- Result: flares in 14% (RZV) vs 15% (placebo) — difference −1.2% (95% CI −4.7% to 2.2%) — meeting non-inferiority. RZV did not increase short-term flare risk.
- Reactogenicity was higher with RZV than placebo, but — notably — lower in IRD patients than in healthy controls; serious adverse events were rare and similar across groups.
- Limitation: not powered for clinical HZ endpoints or long-term outcomes.
B) Valentini et al — Italian retrospective real-world cohort
114 adults with IRD (RA, spondyloarthritis, connective tissue diseases, vasculitis) vs 65 general-care controls; therapy mix included 33% bDMARD monotherapy, 27% JAK inhibitors, 10% csDMARD monotherapy, 8% mycophenolate, 28% GC only.
- Primary endpoint: HZ recurrence before vs after vaccination, per 100 patient-years.
- Result: HZ relapse fell from 9.29 to 0.45 episodes per 100 patient-years — IRR 0.0484 (95% CI 0.0024–0.965, p<0.001), an ~95% relative reduction. Only one recurrence occurred (14 weeks after dose 2).
- Adverse events were mostly mild/transient (17.5% after dose 1, 14.9% after dose 2 — similar to or lower than controls). Only one patient (PsA) had a clinically meaningful flare needing GC. Safety/effectiveness did not differ by JAK inhibitor or bDMARD use.
C) SLE claims-based cohort (Mayer et al)
2284 RZV-vaccinated SLE patients vs 9020 matched unvaccinated controls (Medicare); 1308 vs 5004 (commercial insurance).
- HZ incidence 5.9 vs 19.8 per 1000 PY in Medicare → vaccine effectiveness 70% (95% CI 50–82%).
- HZ incidence 7.4 vs 16.3 per 1000 PY in commercial cohort → effectiveness 54% (95% CI 18–74%).
Therapy-Specific Effects on Immunogenicity
An under-appreciated nuance — drug class shapes the vaccine response:
- Rituximab / B-cell depletion: profoundly impairs humoral responses (one of the strongest negative predictors), though cellular immunity is often preserved or only moderately reduced.
- JAK inhibitors: can attenuate both arms via IFN/cytokine interference — but real-world data are reassuring (a prospective RA study found no significant impairment; an upadacitinib substudy showed satisfactory humoral responses in ~88% of RA patients on background MTX).
- Glucocorticoids & methotrexate: both suppress immunogenicity; effect is dose/exposure-related for MTX, and stronger primarily at higher GC doses. Low-dose GC (≤5–7.5 mg prednisone equivalent) appears to have minimal impact.
- TNF and most cytokine inhibitors: generally less pronounced reduction than B-cell depletion or JAK inhibition.
- Abatacept: intermediate-to-pronounced attenuation via CD28 co-stimulation blockade — a pilot RCT showed reduced humoral (42%) and especially cellular (10%) responses, although the vaccine remained safe.
The Flare Question — Balanced Interpretation
This is the section most relevant to day-to-day counselling, and the review deliberately weighs conflicting evidence:
Pharmacovigilance signal (Liu et al, VAERS, 2017–Q3 2024): among 920 autoimmune patients, 78 reported flares — an 8.5% flare incidence with a 3-fold increased reporting OR (ROR 3.00, 95% CI 2.40–3.75). Disease-specific RORs were highest for SLE (7.50), MS (5.61) and RA (5.03). 59% of flares occurred within 3 days of vaccination (an early-onset pattern consistent with strong innate activation); no association with age, sex or dose number.
Reassuring cohort/RCT data:
- Leung et al (>45,000 adults ≥50y with IMID): no significant increase in flares within 30 days of either dose.
- Rayens et al (1926 vaccinated vs 5746 unvaccinated RA patients ≥50y): no increased RA flare within 30 days — rate ratio 1.02 (95% CI 0.75–1.37); ~60% effectiveness against HZ and ~90% against PHN.
- Hawkins et al (RA on abatacept RCT): RA flare 68% vs 64% — no additional safety signal.
- SLE claims data: HR for severe SLE flares within 90 days comparable between vaccinated and unvaccinated.
Methodological reading: pharmacovigilance is useful for signal detection but is subject to reporting bias; observational cohorts give more reliable incidence estimates; RCTs (least confounded) show no increased short-term flare risk. Overall, the evidence does not support a clinically meaningful increase in flare risk — though mild, early flares may occur in a susceptible minority, with SLE the group warranting most caution.
Guideline Landscape
- EULAR (2019): recommends HZ vaccination in high-risk IRD; wording still reflects the ZVL era but now implicitly favours RZV.
- ACR (2022): strongly recommends RZV for adults on immunosuppression (including JAK inhibitors, B-cell depleting agents, csDMARDs); ideally before initiating B-cell depletion.
- ACIP (2022): endorses two RZV doses for adults ≥19 years who are/will be immunosuppressed; standard interval 2–6 months, shortened to 1–2 months if rapid protection is needed.
- STIKO (Germany): RZV routine for all adults ≥60 years and — newly, from late 2025 — an indication vaccination from age ≥18 years for those at increased HZ risk, including IRD.
The Implementation Gap (Coverage)
Despite clear recommendations, uptake is poor:
- German single-centre IRD cohort: only 13.1% ever received a zoster vaccine (vs influenza 68.5%, pneumococcal 34.7%).
- Israeli nationwide study (>14,000 RA/PsA/SLE patients): RZV coverage 3.6% — lowest in younger, less comorbid (but still high-risk) patients.
- US claims (2018–2019): only 14.8% of commercially insured and 43.2% of Medicare beneficiaries ≥50y with IMID had ≥1 dose; series completion among initiators was high (76–85%).
Cited barriers: rheumatologist time constraints, competing priorities, and uncertainty over who is responsible for vaccination. Suggested fixes: EHR best-practice alerts, shared rheumatology–primary care pathways, patient education and portal reminders.
Practical Timing Strategy
The review’s Table 1 — suggested timing of RZV in adults with IRD according to immunosuppressive therapy:
| Drug | HZ risk | RZV recommendation | Suggested timing | Treatment hold? | Evidence |
|---|---|---|---|---|---|
| csDMARDs (MTX, leflunomide, sulfasalazine) | Moderate | Strongly recommended in all patients ≥50 years; consider from 18 years if additional risk factors | Any time; ideally during stable disease | Individually consider 1–2 week MTX-hold after each dose in stable RA | ACR guideline; MTX-hold extrapolated from influenza and pneumococcal vaccination data in MTX-treated patients (moderate certainty for MTX-hold) |
| Cytokine inhibitors (TNF, IL-6, IL-17, IL-23 inhibitors, T-cell co-stimulation inhibitor) | Moderate | Strongly recommended | Any time during maintenance therapy | No routine hold | No signals for serious immune-mediated events in RZV trials and IRD cohorts; ACR/ACIP allow vaccination on therapy (moderate certainty) |
| Abatacept | Moderate | Strongly recommended | Preferably vaccinate before treatment | Individually consider 1 week abatacept-hold before and after each dose in stable RA | ACR guideline, DGRh recommendations (low certainty for hold) |
| JAK inhibitors | High | Prioritise RZV irrespective of age in long-term users | Preferably before or early after JAKi start; if already on JAKi, vaccinate without interruption | No routine hold; consider individualised approach in unstable disease | Markedly increased HZ risk under JAKi; no evidence that short JAKi holds improve immunogenicity (low–moderate certainty for timing or hold) |
| B-cell-depleting therapies (rituximab, obinutuzumab) | High | Strongly recommended before or between cycles | Ideally complete 2 doses ≥2 weeks before first infusion; if already on treatment, vaccinate mid-cycle (≥4–6 months after last and ≥4 weeks before next infusion) | No evidence-based hold; adjust timing rather than stopping the therapy | B-cell depletion blunts humoral responses; transplant and RA data support mid-cycle vaccination strategy (moderate certainty, timing adjustments rather than holding) |
| High-dose glucocorticoids (≥10–20 mg prednisolone equivalent) | High | Strongly recommended regardless of age | If possible, vaccinate when dose is being tapered | No routine hold (risk of disease flare outweighs potential benefit) | High GC-associated HZ risk; RZV is safe under GCs (low–moderate certainty) |
| Combination immunosuppression (csDMARD + bDMARD + GC) | High | Strongly recommended; consider prioritising even in 18–49 years | Preferably before escalation to combination therapy or during most stable phase | No routine hold; individualised decisions | Highest HZ risk in combination regimens; benefit–risk ratio most favourable (low certainty, evidence largely extrapolated from heterogeneous cohorts and the incremental effects of combined therapies) |
General principles: vaccinate during low/moderate disease activity; counsel on common local/systemic reactions in the first 72 hours and the small flare risk (especially SLE); consider short-term monitoring (telemedicine or brief visit) for 3–7 days after each dose in high-activity, prior-severe-flare or complex-combination patients. Allow ≥2 weeks between dose 2 and starting therapy where feasible.
Review Limitations the Paper Acknowledges
- The pivotal phase 3 trials excluded most immunosuppressed patients; extrapolation to IRD relies on smaller, often heterogeneous cohorts.
- The Italian cohort is single-centre, small, and a pre–post comparison without a control group — vulnerable to regression to the mean and residual confounding.
- Claims-based studies (SLE and other IRDs) rely on administrative definitions of flare and HZ, risking outcome misclassification and lacking clinical detail.
- The Brazilian phase 4 RCT, while robust for short-term safety, was not powered for clinical HZ endpoints or long-term outcomes.
- Drug-specific immunogenicity data (B-cell depletion, JAK inhibitors, combinations) come largely from small cohorts with non-standardised endpoints.
- Long-term durability under chronic immunosuppression is unknown — protection may plausibly wane faster than the ≥10 years seen in immunocompetent adults.
Key Takeaways
- RZV works in IRD. Across an RCT and real-world cohorts, RZV delivers substantial protection — a marked ~95% reduction in HZ recurrence in routine care, and 54–70% effectiveness even in SLE.
- Short-term flare risk is not increased in RCT and large cohort data. The pharmacovigilance ROR signal (notably SLE) reflects reporting-biased signal detection — it argues for informed consent and short-term monitoring, not vaccine avoidance.
- Cellular immunity matters more than antibodies. Robust CD4+ T-cell responses are often preserved even when humoral responses are blunted — serology alone underestimates protection.
- Therapy class shapes the response. Rituximab and abatacept most impair vaccine responses; JAK inhibitors are a paradox (highest HZ risk but generally adequate immunogenicity); low-dose GC has minimal effect.
- Timing should be individualised, but vaccination should rarely be delayed. Complete RZV before B-cell depletion or treatment escalation where possible; otherwise vaccinate on therapy without routine drug holds.
- The real problem is under-vaccination. Coverage of 3.6–14.8% in high-risk IRD populations, worst in younger patients, is the dominant clinical gap — system-level reminders and clear responsibility assignment are needed.
- Priority groups for proactive RZV: patients ≥50 years; any age on JAK inhibitors, high-dose GC or combination immunosuppression; prior HZ; multiple comorbidities or malignancy.
- Open research questions: durability and booster timing under heavy immunosuppression, predictive biomarkers (B-cell reconstitution, interferon signatures), disease-specific immunogenicity studies, long-term flare characterisation, and IRD-tailored cost-effectiveness analyses.
Bottom line for practice: For most patients with IRD on immunosuppressive therapy, the benefit of RZV clearly outweighs the small risk of a short-term, usually mild and self-limited flare. The clinical task is no longer deciding whether to vaccinate, but ensuring it actually happens — with sensible timing and brief post-dose vigilance in the highest-activity patients.