TL;DR: In the first double-blind RCT of mechanism-of-action switching after a first TNFi fails, switching to upadacitinib beat cycling to adalimumab at 12 weeks — roughly doubling low-disease-activity rates and winning on the primary endpoint and 4 of 5 ranked secondaries — but function (HAQ-DI) did not separate, the strictest CRP-independent remission targets favoured it only numerically, and safety was comparable. (Industry-sponsored; 12-week data.)
The Clinical Problem
TNF inhibitors remain the most common first advanced therapy in RA, yet up to 50% discontinue within 1–4 years, mostly for inefficacy or intolerance. When the first TNFi fails, the fork in the road is:
- Cycle to a second TNFi (still done in 46–64% of patients in real-world data), or
- Switch mechanism of action (MOA) to a drug that works differently.
Registry and cross-sectional data hint that MOA switching gives better disease control, higher persistence, and lower cost — but the evidence base was largely observational. Critically, no RCT had ever tested switching to a JAK inhibitor after first TNFi failure. Guidance also diverges: ACR conditionally favours MOA switching, whereas EULAR leaves cycling vs switching open (JAKi permitted after risk assessment).
The Research Question
In patients with active RA despite a first (non-adalimumab) TNFi, is switching to the JAKi upadacitinib more efficacious than cycling to a second TNFi (adalimumab) at 12 weeks — on a background of stable methotrexate?
How the Study Was Designed
Population (218 sites, 24 countries; enrolled Jun 2023–Jun 2025)
- Adults, RA ≥3 months (2010 ACR/EULAR criteria)
- Prior treatment ≥3 months with a single non-ADA TNFi (certolizumab, etanercept, golimumab, or infliximab; originator or biosimilar)
- Ongoing active disease OR discontinuation for intolerance (up to 15% could be the intolerant subgroup)
- Active disease at entry: ≥6 swollen (of 66), ≥6 tender (of 68), hs-CRP ≥3 mg/L
- Stable MTX 15–25 mg/wk (lower floors if intolerant / in China, Japan, Korea)
- Excluded: prior JAKi, prior ADA, or any non-TNFi biologic/tsDMARD; JIA; other inflammatory arthritis
Randomisation & blinding (1:1, double-dummy)
- UPA 15 mg once daily (oral) + placebo SC injection
- ADA 40 mg every 2 weeks (SC, originator) + placebo tablet
- Prior TNFi cleared via a protocol washout (a design choice that matters — see limitations)
- 12-week double-blind period; blinded extension to 48 weeks ongoing
Endpoints
- Primary: DAS28-CRP ≤3.2 at week 12 (superiority) — CRP-based because CRP was run in a central lab to avoid inter-site ESR variability, and to align with EMA requirements.
- Ranked secondary (tested by a step-down gatekeeping procedure at α = 0.05; a lower-ranked endpoint could only be declared significant if every endpoint above it passed): (1) ACR50, (2) DAS28-CRP <2.6, (3) change in DAS28-CRP, (4) change in pain (0–10 NRS), (5) change in HAQ-DI.
Statistics
- Target N = 480 for ≥90% power to detect a 15% difference, assuming an ADA response of ~23%.
- 492 randomised; 1 received no drug → 491 in the full analysis set.
- Conservative imputation: non-responder imputation for binary endpoints; multiple imputation with return-to-baseline for continuous endpoints; post-rescue visits treated as failures/baseline.
The Results
Who was studied (baseline)
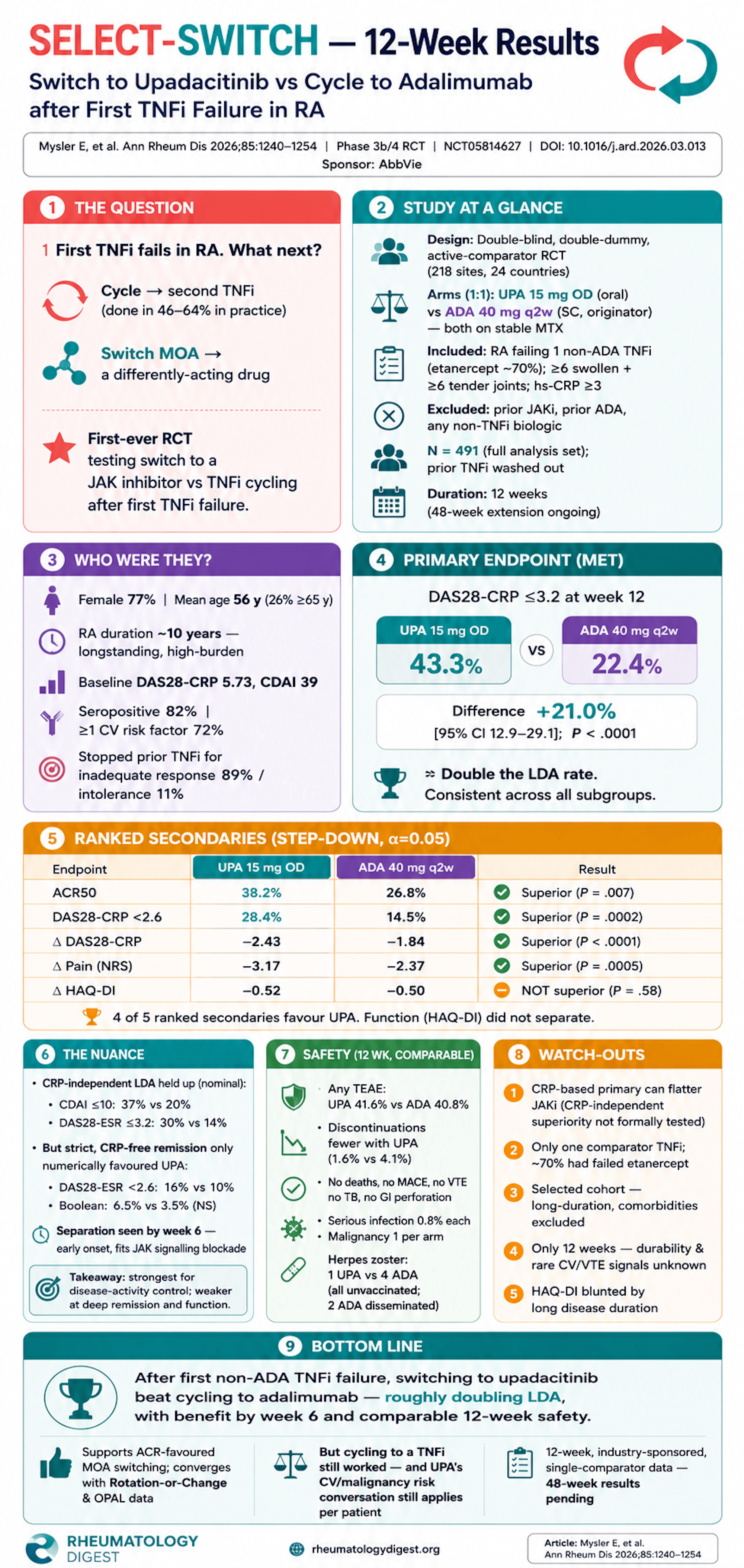
- 77.4% female, mean age 55.6 y (26.3% ≥65 y), RA duration ~10.2 y — a longstanding, high-burden cohort.
- High activity: mean CDAI 38.98, DAS28-CRP 5.73.
- 81.8% anti-CCP and/or RF positive; 72.1% had ≥1 CV risk factor; 40.5% on oral steroids.
- Prior TNFi was etanercept in ~70%; discontinuation was for inadequate response in 89.4% (of these, 54.9% primary / 45.1% secondary non-responders) and intolerance in 10.6%.
Primary endpoint — met
- DAS28-CRP ≤3.2: UPA 43.3% vs ADA 22.4%; difference 21.0% [95% CI 12.9–29.1]; P < .0001 — roughly double the low-disease-activity rate. Consistent across all baseline subgroups.
Ranked secondary endpoints
- ACR50: 38.2% vs 26.8%; diff 11.4% [3.1–19.6]; P = .0068 ✅
- DAS28-CRP <2.6 (remission-range): 28.4% vs 14.5%; diff 13.9% [6.7–21.1]; P = .0002 ✅
- Δ DAS28-CRP: −2.432 vs −1.840; diff −0.593; P < .0001 ✅
- Δ Pain (NRS): −3.165 vs −2.373; diff −0.792; P = .0005 ✅
- Δ HAQ-DI: −0.523 vs −0.496; diff −0.027; P = .5849 ❌ NOT superior
Non-ranked / nominal endpoints (favouring UPA)
- CRP-independent LDA held up: DAS28-ESR ≤3.2 29.8% vs 14.2%; CDAI ≤10 36.7% vs 19.9%; SDAI ≤11 38.1% vs 20.7% (all nominal P < .0001).
- SDAI ≤3.3 remission: 8.9% vs 4.0% (P = .0251); ACR20 67.7% vs 55.4%; ACR70 18.8% vs 9.3%.
- FACIT-Fatigue improvement +9.4 vs +7.7.
- Separation emerged by week 6 for DAS28-CRP ≤3.2, ACR50, and pain — in keeping with the faster onset expected from intracellular JAK signalling blockade vs cytokine neutralisation.
The nuance to foreground: the stricter, CRP-independent remission endpoints (DAS28-ESR <2.6 15.9% vs 10.2%; CDAI ≤2.8 8.6% vs 4.5%; ACR/EULAR Boolean 6.5% vs 3.5%) were numerically favourable but not statistically significant. The gap between arms narrows as the bar is raised and as CRP is removed from the metric.
Safety (12 weeks) — broadly comparable
- Any TEAE: UPA 41.6% vs ADA 40.8%; serious 2.0% vs 2.4%.
- Discontinuation for TEAE was lower with UPA (1.6% vs 4.1%).
- No deaths, no MACE, no VTE, no active TB, no GI perforation.
- Serious infections 0.8% each; 2 malignancies total (1 per arm).
- Herpes zoster: 1 UPA vs 4 ADA — all 5 patients unvaccinated; 2 ADA cases were disseminated with postherpetic neuralgia (a reminder that zoster risk is not JAKi-exclusive, and that vaccination gaps persisted here).
Study Limitations
- CRP-anchored primary endpoint favours JAKi. JAK inhibition lowers CRP directly, so DAS28-CRP/SDAI can flatter UPA. Formal superiority testing on CRP-independent measures (CDAI, DAS28-ESR) was not prespecified as ranked — so those reassuring results are nominal only.
- Only one comparator TNFi. ADA-intolerant/resistant patients were excluded, so ~70% had failed etanercept. Generalisability to other cycling scenarios is uncertain.
- Selected population. Long disease duration, high inflammatory load, significant comorbidities excluded — not fully representative of all first-TNFi-failure patients under strict treat-to-target (though registries confirm T2T is often under-applied in practice).
- Short horizon. 12 weeks captures early treatment only; 48-week durability and long-term safety are pending. The sample size/duration also limit any read on rare CV/VTE signals.
- HAQ-DI did not separate — likely because HAQ-DI responsiveness falls with longer disease duration, and both arms improved meaningfully (a pattern echoed in Rotation or Change and SELECT-CHOICE).
How This Study Adds to Practice
- First global double-blind RCT to test MOA switching (to a JAKi) vs TNFi cycling after first TNFi failure — filling a gap left by SELECT-COMPARE and SELECT-CHOICE.
- Provides RCT-grade support for the ACR-favoured strategy of switching MOA, converging with the Rotation or Change trial (non-TNFi biologic > second TNFi at wk 24) and the OPAL registry (JAKi switch > cycling at 3 months).
- Reinforces that cycling to a second TNFi is not futile — ADA still produced real responses (its DAS28-ESR ≤3.2 rate mirrored EXXELERATE) — but switching to UPA outperformed it across multiple domains.
- Decision-making caveat for the clinic: the benefit must be balanced against UPA’s risk profile in older patients and those with CV or malignancy risk factors (a large share of this cohort). Notably, ADORRA-SWITCH found ADA trough-level–guided switching was not superior to random switching — so drug-level monitoring is not (yet) a way to personalise this choice.
Final Take-Aways
- After failing a first non-ADA TNFi, switching to upadacitinib beat cycling to adalimumab on the primary endpoint and 4 of 5 ranked secondaries — roughly doubling LDA rates by week 12.
- Benefit appeared early (by week 6) and was consistent across subgroups.
- HAQ-DI (function) did not separate, and the strictest CRP-independent remission targets favoured UPA only numerically — interpret the “superiority” as strongest for disease-activity control, more modest at deep remission and physical function.
- Safety was comparable at 12 weeks, with fewer discontinuations on UPA and no MACE/VTE signal — but the CV/malignancy risk conversation still applies to individual patients.
- This is 12-week, industry-sponsored, single-comparator data; 48-week extension results will decide how durable the advantage is.