TL;DR: B cells are the single through-line of Sjögren disease — linking the autoantibodies, glandular pathology, the highest lymphoma risk of any autoimmune disease, and the entire emerging drug pipeline — so endotyping by B-cell activity may identify both who develops lymphoma and who responds to B-cell-targeted therapy, with newer BAFF/APRIL, CD40L, BTK and FcRn agents now succeeding in phase II where rituximab failed.
The Clinical Problem
Sjögren disease (SjD) is roughly as common as rheumatoid arthritis, yet it has no FDA-approved disease-modifying therapy. Two intertwined problems explain that gap, and this review argues both trace back to B cells.
- Heterogeneity. SjD ranges from mild sicca to organ-threatening disease. 30–50% of patients have extraglandular involvement (haematologic, pulmonary, renal, neurologic). Serologic abnormalities typically predate diagnosis and are stable over time, but the natural history of organ involvement is highly variable — which makes prognosis, trial design, and treatment planning very difficult.
- Lymphoma. SjD carries the highest lymphoma risk of any autoimmune disease, and this risk is not evenly distributed across patients — it clusters in the B-cell-active subgroup.
The authors’ organising claim: if we can endotype SjD by B-cell activity, we can simultaneously identify who will develop lymphoma and who will respond to B-cell-targeted therapy.
The Anchoring Case (Worth Teaching in Full)
- 39-year-old woman, 15-year history of SjD complicated by leukocytoclastic vasculitis and inflammatory arthritis.
- One year of recurrent parotid swelling; extensive dental work.
- ESSPRI 3 (i.e., relatively low symptom burden). Prior pregnancy complicated by congenital heart block.
- Unstimulated salivary flow 0.03 mL/5 min (normal >0.5); Schirmer’s normal (17 and 35 mm/5 min).
- Bilateral parotid enlargement (3 cm); no cervical lymphadenopathy; no synovitis but tender MCPs/PIPs.
- ANA, anti-Ro/SSA, anti-La/SSB, RF all positive. Normal CBC, metabolic panel, anti-CCP.
- Salivary gland ultrasound: diffuse hypoechoic and anechoic foci.
- Core needle parotid biopsy: lymphoepithelial lesions + germinal-centre-like structures, no lymphoma. Flow cytometry negative for monoclonality.
- Started hydroxychloroquine; advised 6-month follow-up.
Nine years later, after being followed only by ENT for recurrent parotid swelling and undergoing repeated cyst drainage, she was referred for parotidectomy — pathology showed MALT lymphoma. The teaching point is uncomfortable and deliberate: every red flag was present at the first visit, and she was lost to rheumatology follow-up.
Endotyping — From Phenotype to Pathobiology
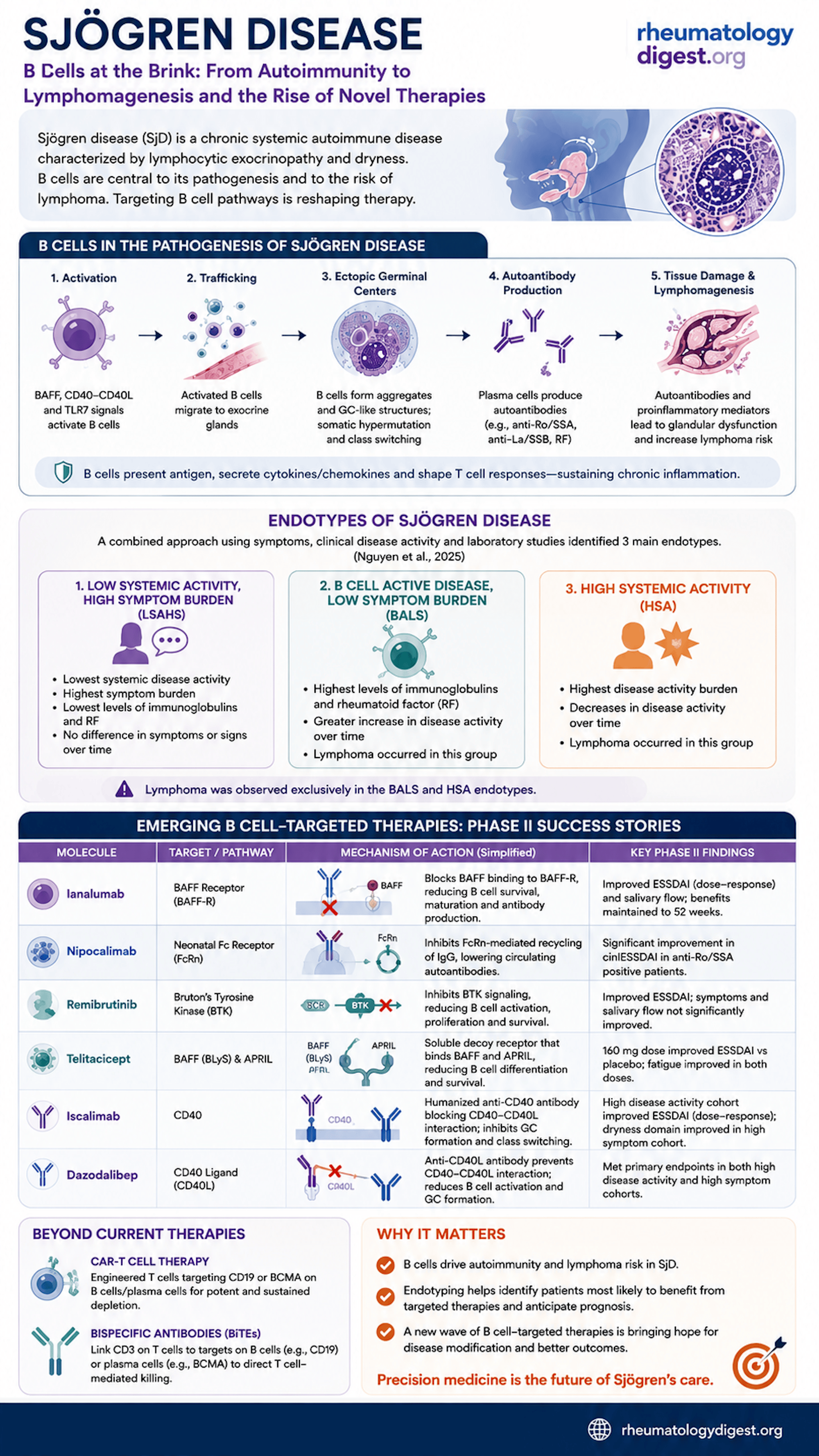
Endotypes are pathobiologically similar subgroups. Approaches to date have ranged from symptom-based clustering to blood transcriptomics/proteomics and glandular transcriptomics. The review foregrounds Nguyen et al, who combined symptoms, clinical disease activity, and routine labs to derive three endotypes:
| Endotype | Character | Trajectory | Lymphoma |
|---|---|---|---|
| LSAHS — low systemic activity, high symptom burden | Highest symptom burden; fewest lab abnormalities | Stable over time | Not observed |
| BALS — B-cell active, low symptom burden | Highest immunoglobulins and RF (the case patient) | Disease activity increases over time | Yes |
| HSA — high systemic activity | Highest disease activity burden | Disease activity decreases over time | Yes |
The critical observation: lymphoma occurred exclusively in the BALS and HSA groups. The BALS patient — serologically loud but symptomatically quiet — is precisely the patient a busy clinic is most likely to under-monitor.
Caveat the authors are explicit about: endotypes are not yet ready for clinical deployment. Longitudinal natural-history studies, prospective validation in independent cohorts, and evidence that endotype can select therapy are all still needed.
Why B Cells Sit at the Centre
- Genetics: GWAS implicate B-cell genes — PRDM1, TNFAIP3, BLK, CXCR5.
- Peripheral compartment: Plasmablasts are increased and correlate with autoantibody levels, disease activity, and lymphoma risk. Circulating memory B cells are decreased — but are increased in the salivary glands, implying trafficking to target tissue.
- Glandular compartment: 10–30% of patients have germinal-centre-like structures in salivary glands. Bona fide GCs express AID and CXCR5; B-cell aggregates do not — but both contain autoreactive B cells. An increased intraglandular IgG:IgA-producing B-cell ratio correlates with focus score.
- Atypical memory B cells (human) / age-associated B cells (mouse) — proinflammatory subsets linked to systemic autoimmunity — are found in SjD; their pathogenic role is still being worked out.
- Signalling and survival: BTK is elevated in SjD B cells. BAFF is elevated in serum and salivary gland. BAFF-transgenic mice develop sialadenitis and have increased lymphoma risk.
- A conceptual shift worth flagging: BAFF is secreted not only by myeloid cells but by salivary gland epithelial cells themselves. The glandular epithelium is therefore an active driver of B-cell activation, not a passive victim of it.
When B Cells Go Rogue — Lymphomagenesis
The numbers:
- NHL affects 5–10% of SjD patients and contributes materially to mortality.
- Risk is 5 to >20 times that of the general population — the highest among all autoimmune diseases (the wide range reflects cohort heterogeneity).
- 98% of SjD-associated lymphomas are of B-cell origin.
- >90% are MALT lymphoma or DLBCL. Low-grade MALT is the commonest, with the salivary gland as primary extranodal site in 70% (also lung, stomach, ocular adnexa).
The mechanism: chronic antigenic stimulation drives polyclonal B-cell expansion; acquisition of driver mutations then permits monoclonal proliferation. Two mechanistic details worth carrying away:
- Singh et al (single-cell DNA/RNA sequencing in SjD cryoglobulinaemic vasculitis) showed that RF-producing B cells acquire lymphoma driver mutations before the V(D)J mutations that convert benign RF into pathogenic RF. In other words, the oncogenic hit may be what lets an autoreactive clone escape tolerance checkpoints in the first place — a mechanistic bridge explaining why cryoglobulinaemic vasculitis and lymphoma travel together.
- TNFAIP3/A20: functional abnormalities were found in 77% of SjD patients with MALT lymphoma and 29% of those with other lymphoma histologies.
Clinical predictors — four cohorts, one recurring signal:
| Cohort | Size (LPD/NHL events) | Predictors identified |
|---|---|---|
| Ioannidis et al | 723 (38) | Parotid enlargement, palpable purpura, low C4 |
| Baimpa et al | 536 (40) | Neutropenia, cryoglobulinaemia, splenomegaly, lymphadenopathy, low C4 |
| Quartuccio et al | 661 (40) | Cryoglobulins, anti-La/SSB, leukopenia, low C4 |
| Fragkioudaki et al | 381 (92) | Salivary gland enlargement, lymphadenopathy, Raynaud, anti-Ro/anti-La, RF, monoclonal gammopathy, low C4 |
Low C4 appears in all four. Add to these: high focus score and germinal centres on labial salivary gland biopsy; high systemic disease activity; and imaging — parotid PET-CT SUVmax ≥4.7, and OMERACT salivary gland ultrasound grade 2–3 (hypoechoic/anechoic lesions), which is where parotid lymphomas tend to arise.
MALT lymphoma characteristically announces itself as recurrent or persistent salivary gland swelling. B symptoms, lymphadenopathy, or recurrent parotitis in a high-risk serologic profile warrant evaluation; ultrasound or CT/PET can direct the biopsy site.
The Therapeutic Landscape
Why rituximab failed. The TEARS and TRACTISS RCTs both missed their primary endpoints. Proposed explanations: overly broad inclusion criteria, endpoints insensitive to change, and — mechanistically important — rituximab may not adequately deplete B cells within salivary gland tissue.
Why the new trials are succeeding. Inclusion criteria have evolved: most now require moderate-to-high systemic activity (ESSDAI) and anti-SSA positivity. This is, in effect, informal endotyping — enriching for the B-cell-active patient.
Successful phase II trials:
- Dazodalibep (anti-CD40 ligand) — the only agent tested prospectively in two distinct endotype-like cohorts, and it met the endpoint in both:
- High activity cohort (ESSDAI ≥5): ESSDAI −6.3 ± 0.6 vs placebo −4.1 ± 0.6, p = 0.0167
- Low activity / high symptom cohort: ESSPRI −1.8 ± 0.2 vs −0.5 ± 0.2, p = 0.0002
- Salivary flow did not improve in either group.
- Ianalumab (anti-BAFF receptor): placebo-adjusted ESSDAI at 300 mg −1.92 (95% CI −4.15 to −0.32); dose–response met (p < 0.025 in four of five models). Improves salivary flow but no clear symptom benefit. Efficacy maintained at 52 weeks.
- Telitacicept (BAFF + APRIL): 160 mg −4.3 (90% CI −7.0 to −1.6), p = 0.002; the higher 240 mg dose was not significant (−2.7; p = 0.056). Fatigue improved at both doses.
- Nipocalimab (anti-FcRn; blocks IgG recycling → lowers circulating autoantibodies): 15 mg/kg clinESSDAI −2.65 (90% CI −4.03 to −1.28), p = 0.002; 5 mg/kg not significant (p = 0.681). [DAHLIAS]
- Remibrutinib (BTK inhibitor): ESSDAI −2.86 (95% CI −4.71 to −1.01), p = 0.003; no significant improvement in symptoms or salivary flow.
- Iscalimab (anti-CD40): high-activity cohort met dose–response endpoint (150 mg −3.0; 600 mg −2.9). High-symptom cohort missed its ESSPRI endpoint (−0.57; CI crosses zero) but improved the ESSPRI dryness domain.
A pattern the review invites you to notice: almost every agent moves ESSDAI (systemic activity) but few move symptoms or salivary flow. Dazodalibep is the exception — and it is also the one that stratified by endotype.
On the horizon:
- CAR-T — CD19-directed (B-cell depletion; efficacy shown in lupus nephritis) and BCMA-directed (plasma cell depletion). Both are rational in SjD given the central roles of B cells and plasma cells. CAR technology is also being explored to generate regulatory cell products.
- Bispecifics / BiTEs — blinatumomab (CD3/CD19; used in 6 RA patients) and teclistamab (CD3/BCMA; used in 5 patients with systemic autoimmunity including SjD, with improvement in all).
- Why these may succeed where rituximab did not: CAR-T, bispecific and BiTE therapies achieve more potent and sustained depletion than CD20-targeted antibodies, and reach plasmablasts, early plasma cells, and memory B cells — both in the periphery and within end organs. That last point maps directly onto rituximab’s suspected failure to clear the glandular compartment.
Key Takeaways
- B cells are the through-line of SjD — they connect the autoantibodies, the glandular pathology, the lymphoma risk, and the entire emerging drug pipeline. This is one disease mechanism, not four separate stories.
- Endotype predicts destiny. Lymphoma occurred exclusively in the B-cell-active (BALS) and high-systemic-activity (HSA) endotypes. The BALS patient — high Ig and RF, low symptom burden — is the one most easily under-monitored, and is exactly the patient in the case.
- Recurrent or persistent parotid swelling is the cardinal warning sign of MALT lymphoma; salivary glands are the primary extranodal site in 70%.
- Low C4 is the single most reproducible lymphoma predictor — it appeared in all four independent risk cohorts. Also weigh: parotid enlargement, palpable purpura, cryoglobulinaemia, RF, lymphadenopathy, monoclonal gammopathy, cytopenias, and germinal centres / high focus score on biopsy.
- Imaging can risk-stratify and target biopsy: OMERACT ultrasound grade 2–3 and parotid PET-CT SUVmax ≥4.7.
- The glandular epithelium is an active participant, secreting BAFF — not an innocent bystander. This reframes SjD as an epithelium-driven B-cell disease.
- Rituximab’s failure was probably not a failure of the B-cell hypothesis — more likely a failure of trial design and of tissue-level B-cell depletion. Newer agents that hit BAFF/BAFF-R, APRIL, CD40–CD40L, BTK and FcRn are now succeeding in phase II.
- Most new agents improve systemic disease activity (ESSDAI), not dryness or symptoms. Manage patient expectations accordingly. Dazodalibep — the one that stratified by endotype — is the notable exception.
- Vigilant, structured surveillance is the practical message of the case. Nine years of ENT-only follow-up for recurrent parotid swelling ended in parotidectomy for MALT lymphoma. Treating SjD-associated lymphoma may, in itself, improve SjD disease activity.
- We are at an inflection point. After decades with no approved disease-modifying therapy, endotype-enriched trials plus deep B-cell depletion (CAR-T, BiTEs) suggest the first real breakthroughs for SjD may be close.