TL;DR: The single biggest lever in SLE pregnancy is planning — conceiving after ≥6–12 months of quiescent disease on pregnancy-compatible therapy, with hydroxychloroquine continued throughout — while the persistence of risk across pregnancies and a long-term cardiovascular signal make SLE pregnancy a lifelong cardiometabolic flag, not just a 9-month event.
The Clinical Problem
SLE predominantly affects women of childbearing age, and as survival and quality of life have improved, more women with SLE are becoming pregnant. Yet pregnancy still carries higher maternal and fetal risk than in the general population, and uniquely, the elevated risk persists across subsequent pregnancies in SLE, whereas healthy women see risk fall as maternal–fetal tolerance matures. Flares and complications cluster in those with active disease at conception, prior lupus nephritis (LN), antiphospholipid syndrome (APS), or recent medication withdrawal. The review covers the bidirectional SLE–pregnancy relationship, the underlying immunobiology, and contemporary peri-conception, pregnancy and lactation care, anchored to the BSR, EULAR and ACR guidelines.
Fertility
- SLE itself does not impair tubal function, but ovarian reserve (AMH) is reduced, particularly after cyclophosphamide. Active disease and renal failure independently impair fertility.
- Cyclophosphamide gonadotoxicity rises with cumulative dose >7.5–10 g or first exposure age >30. The Euro-Lupus regimen (six fortnightly 500 mg pulses) is preferred — low infertility risk under age 30. Consider GnRH analogues for ovarian protection before alkylating agents.
- NSAIDs: evidence for fertility impairment is weak; no need to stop when trying to conceive, though withdrawal can be considered if conception is delayed.
- Family size is smaller in SLE — a Finnish study found childlessness of 9.3% (women) and 4.7% (men).
- Assisted reproduction is safe in well-controlled SLE with thrombotic risk stratification; single-embryo transfer is advised (twins compound preterm risk), and LMWH is used for aPL-positive/obstetric-APS patients during ART.
Contraception
- Oestrogen-containing contraceptives raise VTE risk 2–3 fold, amplified in SLE and especially aPL-positivity → avoid in high-thrombosis-risk or persistently aPL-positive women.
- Copper and progesterone IUDs are safe and not associated with VTE; progesterone-only pills are an alternative. Avoid depot medroxyprogesterone in aPL-positive women. The levonorgestrel IUD is especially useful in those on anticoagulation (minimises menstrual loss).
Impact of Pregnancy on SLE — Flares
- Flares occur in roughly 2.5–35% of pregnancies, mostly 2nd/3rd trimester or early postpartum.
- The Hopkins cohort (398 pregnancies in 304 women) showed higher flare rates in pregnancy and a further rise in the first 3 months postpartum — occurring almost exclusively in women not taking hydroxychloroquine (HCQ).
- Major flare risk factors: HCQ discontinuation, active disease at conception, history of LN, and serologic activity (hypocomplementaemia) in the first trimester.
- Renal relapse is highly remission-dependent: 72% with unplanned pregnancy or incomplete remission vs 11.3% with complete renal remission at conception. Younger age and primigravida status also raise flare risk.
Impact of SLE on Pregnancy — Complications
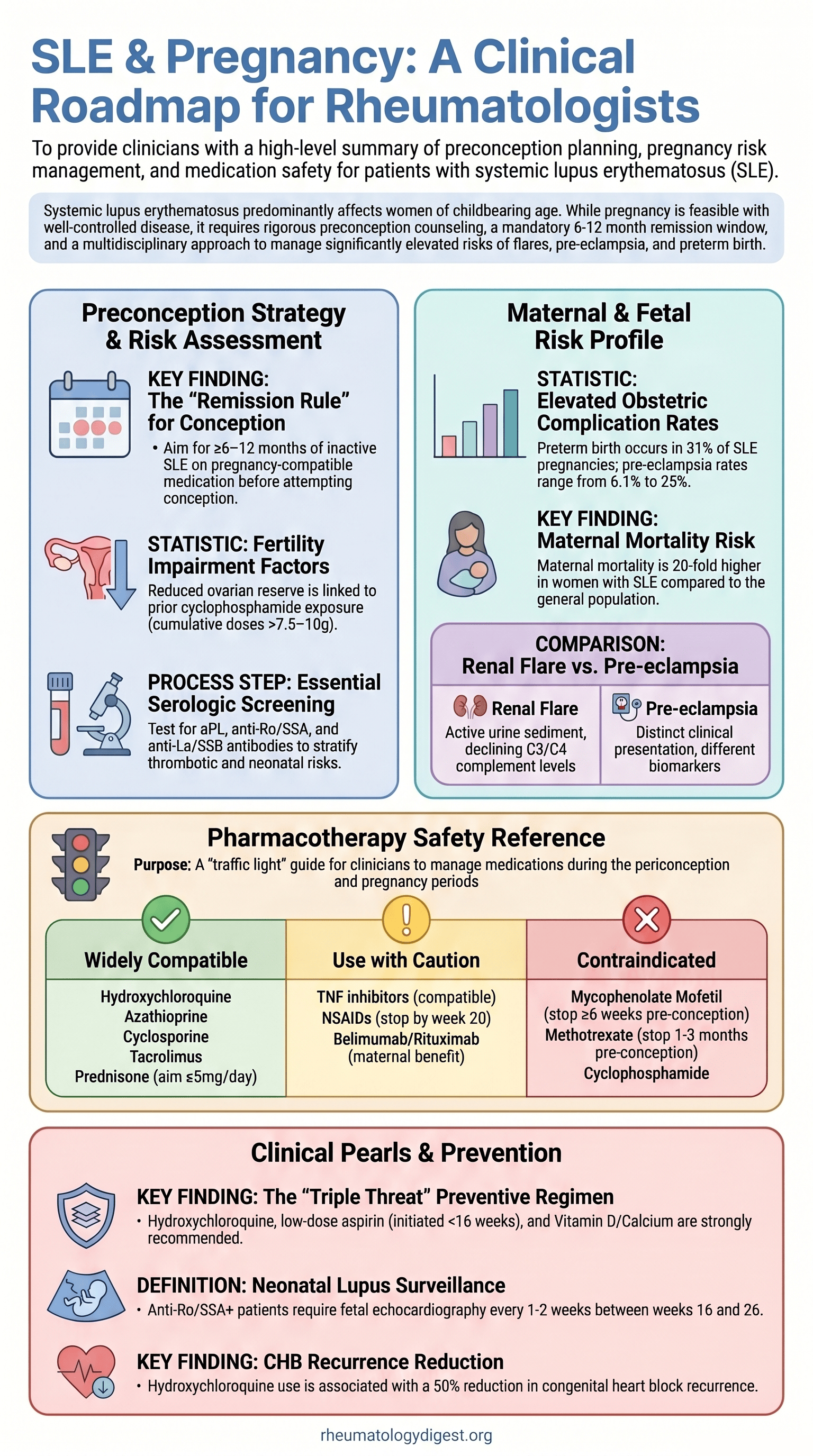
- Maternal mortality is up to 20-fold higher (US population data). Pregnancy loss has fallen from 43% (1960s) to ~17% (early 2000s), approaching the general-population 10–15%.
- Pre-eclampsia: ~5% general vs 6.1–25% in SLE.
- Fetal growth restriction: 5.3% vs 1.6%; small-for-gestational-age 25% vs 4.5%. HCQ reduces FGR.
- Preterm birth: meta-analysis of 8,157 pregnancies → 31% vs 6–10% general; spontaneous preterm via PPROM is twice as common (51% vs 25%).
- Neonatal lupus / congenital heart block (CHB): anti-Ro/La present in ~40% of SLE women; IgG transfer begins at 16 weeks. CHB risk is 1–2% (no prior affected child) rising to 17% after a previously affected child, usually arising in the 2nd trimester and rarely after 26 weeks. CHB carries ~20% mortality, and ~two-thirds of survivors need a pacemaker. HCQ roughly halves CHB recurrence in anti-Ro–positive women with a prior affected infant.
- Long-term: hypertensive disorders of pregnancy in SLE conferred a 2-fold rate of major cardiovascular events and 3-fold incident hypertension at ~11 years (Swedish data) — pregnancy as a cardiovascular “stress test.”
- A Chinese cohort identified a favourable preconception bundle (stable ≥6 months, no active vital-organ disease, on HCQ, prednisone ≤7.5 mg/day) that maximised the chance of a good outcome.
Pathophysiology
- aPL + complement + neutrophils: aPL bind trophoblasts → C5a generation → neutrophil recruitment → NETosis (thrombogenic), ROS and NK recruitment → placental injury. Placentas show increased C3/C4 deposition with circulating complement consumption; C5 is variable. Notably, similar NET/complement findings appear in aPL-negative SLE and in non-SLE pre-eclampsia, implying a broad final common pathway.
- Type I interferon: healthy pregnancy downregulates the IFN signature; in SLE it stays elevated, with the smallest reduction in those who later develop pre-eclampsia/FGR. IFNα drives RSAD2 (lipid accumulation), IFITM (blocks syncytialisation) and CXCL8 (neutrophil recruitment). Caveat: IFNβ in MS doesn’t worsen pregnancy outcomes, and 50–70% of SLE patients have high IFN without complications — so additional drivers must exist.
Preconception Counselling — the Cornerstone
- Aim for ≥6–12 months of quiescent disease on pregnancy-compatible medication before conception, with multidisciplinary care.
- Do not stop pregnancy-compatible drugs (including HCQ) when planning — withdrawal is a common flare trigger. Switch off teratogens onto compatible agents 4–6 months before conception to allow a remission run-in.
- Women with SLE now conceive at a median age in the mid-30s with higher BMI and more ART use. Prepregnancy BMI >25 raised fetal death/preterm risk (HR 3.58, 95% CI 1.45–8.83).
- Test aPL, anti-Ro/SSA, anti-La/SSB for risk stratification. Note the 2023 ACR/EULAR APS criteria are classification, not diagnostic.
Management During Pregnancy
- Care in a combined rheumatology–obstetric clinic; monitor BP, blood and urine; distinguish pre-eclampsia from renal flare (active sediment, falling C3/C4, rising anti-dsDNA favour flare; post-20-week new hypertension, normal complement, raised transaminases favour pre-eclampsia — they can co-exist).
- Fetal echocardiography for anti-Ro/La-positive women from 16–20 weeks, repeated up to 26 weeks; intensified if high-titre anti-Ro or prior CHB.
Pharmacologic pillars:
- Hydroxychloroquine for all — reduces flares, pre-eclampsia, FGR, preterm birth and CHB recurrence. Adherence matters: non-adherent HCQ levels raised preterm odds markedly (OR 11.2, 95% CI 2.3–54.2).
- Low-dose aspirin started before 16 weeks for pre-eclampsia prevention in at-risk women.
- Heparin/LMWH: VTE incidence is far higher in SLE (~62 vs ~7.2 per 10,000 pregnancies; PE adjusted OR 9.76). Thromboprophylaxis should be individualised (e.g. DORIS activity + RCOG model), not blanket. Switch VKA → LMWH at confirmation of pregnancy.
- Adjuncts: folic acid 400 µg, vitamin D 1,000 IU, calcium 1,000 mg. A 2025 Cochrane update found little calcium effect on pre-eclampsia (RR 0.83, 95% CI 0.67–1.04), but it is retained in SLE for bone protection (glucocorticoids, heparin).
Drug-Safety Framework
| Drug / class | Pregnancy | Lactation | Notes |
|---|---|---|---|
| Hydroxychloroquine, chloroquine | ✅ Compatible | ✅ Compatible | Backbone therapy — continue in all; ensure adherence |
| Azathioprine | ✅ Compatible | ✅ Compatible | |
| Ciclosporin, tacrolimus | ✅ Compatible | ✅ Compatible | |
| Colchicine | ✅ Compatible | ✅ Compatible | |
| Prednis(ol)one (non-fluorinated) | ✅ Compatible | ✅ Compatible | Lowest effective dose, aim ≤5 mg/day; watch GDM, preterm birth; plan stress dosing if ≥5 mg >3 weeks |
| Fluorinated steroids (e.g. dexamethasone, betamethasone) | ⚠️ Selected | — | Cross the placenta; reserved for fetal lung maturation |
| NSAIDs | ⚠️ Selected | Agent-dependent | Stop ~20–28 weeks; avoid etoricoxib in lactation |
| Low-dose aspirin | ✅ Compatible | ✅ Compatible | Start before 16 weeks for at-risk women |
| Heparin / LMWH | ✅ Compatible | ✅ Compatible | Individualise thromboprophylaxis; switch VKA → LMWH at confirmation of pregnancy |
| IVIG | ⚠️ Selected | ✅ Compatible | |
| Belimumab | ⚠️ Selected | Limited data | Crosses placenta via FcRn from ~16 weeks |
| Rituximab | ⚠️ Selected | ✅ Compatible | B-cell agents after 20 weeks → transient neonatal B-cell depletion (normalises ~6 months) |
| TNF inhibitors | ⚠️ Selected | ✅ Compatible | |
| Anifrolumab | ❌ Not in pregnancy | ✅ Compatible | Insufficient pregnancy data |
| Methotrexate | ❌ Contraindicated | ⚠️ ≤25 mg/week only if no alternative | |
| Mycophenolate | ❌ Contraindicated | ❌ Avoid | Teratogen — switch 4–6 months pre-conception |
| Leflunomide | ❌ Contraindicated | ❌ Avoid | Cholestyramine washout |
| Cyclophosphamide | ❌ Contraindicated | ❌ Avoid | Gonadotoxic |
| Voclosporin | ❌ Contraindicated | ❌ Avoid | |
| JAK inhibitors | ❌ Contraindicated | ❌ Avoid |
bDMARD note: monoclonal antibodies cross the placenta via FcRn from ~16 weeks. After B-cell-depleting therapy beyond 20 weeks, 2024 EULAR advises avoiding live infant vaccines for the first 6 months. Delay breastfeeding 2–4 h after IV methylprednisolone pulses.
Lactation
- Encourage breastfeeding, though initiation/duration are lower in SLE. Most SLE drugs are compatible; bDMARDs are safe (large molecules, minimal transfer, digested in the infant gut). MTX ≤25 mg/week may be considered if no alternative; delay feeding 2–4 h after IV methylprednisolone pulses.
- Avoid while breastfeeding: cyclophosphamide, mycophenolate, leflunomide, voclosporin, etoricoxib, and JAK inhibitors.
Key Takeaways
- Plan, don’t react. The single biggest lever is conceiving after ≥6–12 months of quiescent disease on pregnancy-compatible therapy, with teratogen switches completed months ahead.
- Hydroxychloroquine is the backbone — flare reduction, lower pre-eclampsia/FGR/preterm rates, and halved CHB recurrence. Continuing it (and ensuring adherence) is non-negotiable; stopping it drives most pregnancy flares.
- Risk stratify by phenotype and antibodies. Prior LN, active disease, hypertension, aPL/APS and anti-Ro/La each define distinct surveillance and prophylaxis pathways (renal monitoring, aspirin, LMWH, fetal echo). Complete renal remission before conception dramatically cuts renal relapse (72% → 11%).
- The persistence of risk across pregnancies and the long-term cardiovascular signal make SLE pregnancy a lifelong cardiometabolic flag, not just a 9-month event.
- Mechanistic gap: the aPL–complement–NET axis and a poorly-downregulated type I interferon signature are leading candidates, but no marker yet reliably predicts who will develop complications — the field is moving toward prospective multiethnic registries, biobanking and placental organoid models.
- Evidence base is thin where it matters most — pregnant women are routinely excluded from trials. Most drug-safety guidance rests on observational data, so shared decision-making remains central.