TL;DR: T-cell engagers — off-the-shelf bispecific antibodies that redirect a patient’s own T cells onto autoreactive B/plasma cells — are a repeatable, dose-adjustable alternative to CAR-T with real but preliminary efficacy across SLE, SSc, RA, myositis and Sjögren’s; the review’s central message is that rheumatology has been under-dosing them relative to oncology, giving incomplete tissue B-cell depletion that likely explains the frequent post-treatment relapses.
The Clinical Problem
B cells sit at the centre of many autoimmune diseases — SLE, systemic sclerosis (SSc), rheumatoid arthritis (RA), idiopathic inflammatory myositis (IIM), and primary Sjögren’s (PSS). Deep B-cell depletion has therefore become an attractive strategy, and CD19 CAR-T has produced striking early results in autoimmunity. But CAR-T is bespoke: complex manufacturing, logistical burden, and high cost restrict access.
T-cell engagers (TCEs) are pitched as the pragmatic alternative — off-the-shelf bispecific antibodies that can be given repeatedly and dose-adjusted, potentially widening access (including to patients far from CAR-T centres). This review asks what the (very early) rheumatology experience actually shows, and — importantly — whether we are dosing these drugs correctly.
What a TCE Is, and How It Works
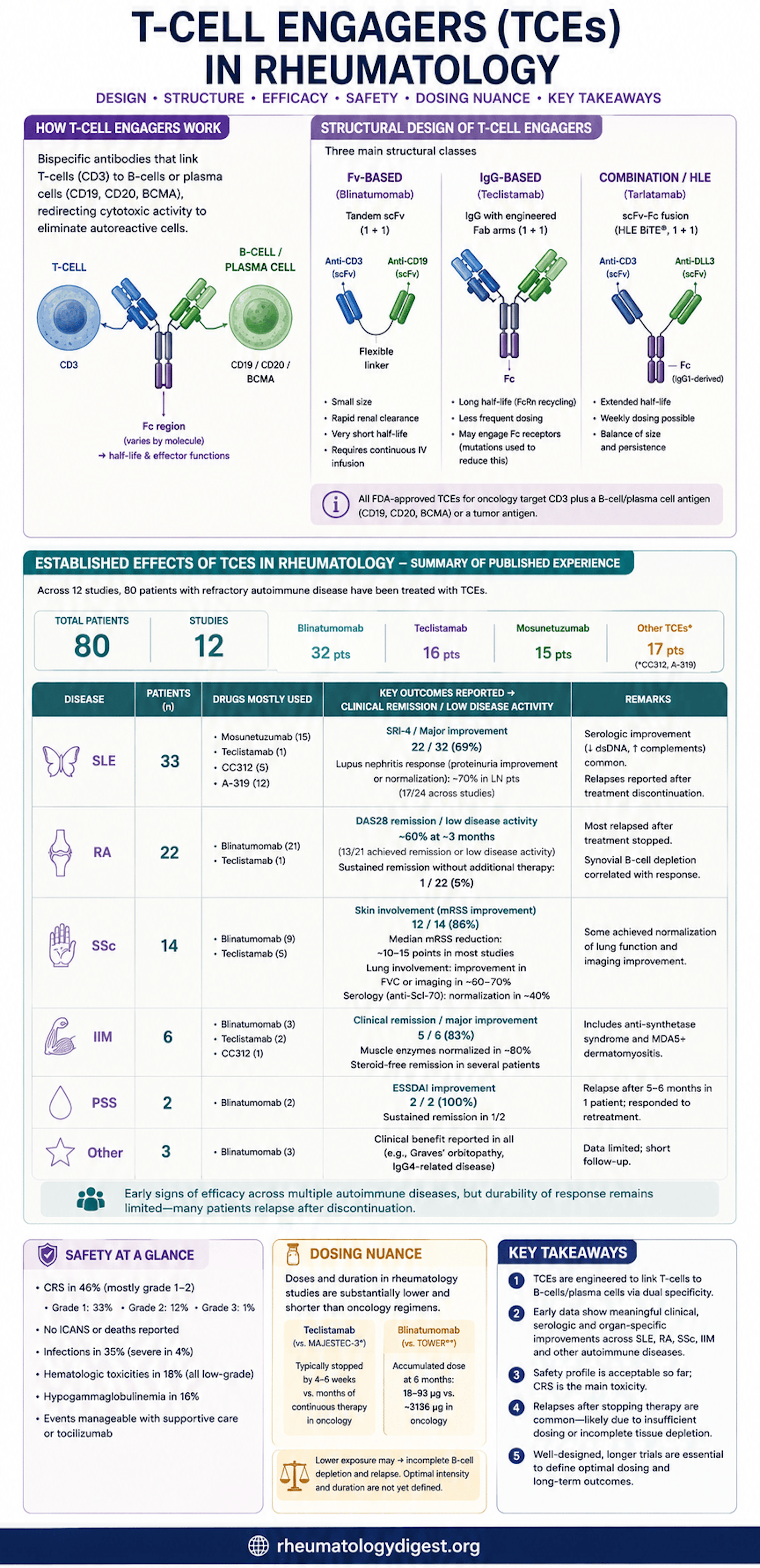
A TCE is a bispecific antibody with one arm against a target-cell antigen (on the B cell or plasma cell) and one arm against CD3 on T cells. By physically bridging the two, it redirects a patient’s own cytotoxic T cell onto the autoreactive B cell, which is then killed via granzymes and perforins, with amplifying cytokine release. Crucially, this needs no genetic engineering of the patient’s cells — the key practical advantage over CAR-T.
Blinatumomab (CD19×CD3) was the first FDA-approved TCE (2014, for r/r B-ALL); as of July 2025 ten TCEs are approved across haematologic and solid cancers.
Structural Diversity (Why It Matters Clinically)
- Format: Most are 1+1 (one CD3 arm, one target arm). 2+1 designs (two target arms) exploit avidity — binding strongly to cells with high antigen density while sparing low-expressing normal cells (e.g. glofitamab). Trispecifics (1+1+1) add a third antigen.
- Backbone → pharmacokinetics:
- Fv-based (e.g. blinatumomab): no Fc, small, good tissue penetration, but renally cleared with a ~2-hour half-life → requires continuous IV infusion.
- IgG-based (e.g. teclistamab, mosunetuzumab): FcRn recycling → long half-life, less frequent (often subcutaneous) dosing. Trade-off: the Fc can engage NK cells/monocytes (ADCC/CDC) and drive off-target activation and CRS, so most are Fc-silenced or IgG4.
- Combination / HLE BiTEs (e.g. tarlatamab, ~5.7-day half-life): weekly dosing, but prolonged exposure can’t be “switched off” like an infusion if toxicity arises.
- Heterodimer engineering (knobs-into-holes, CrossMab, DuoBody) solves the chain-pairing problem — useful background when reading the drug table.
Targets
- CD19 — broadly expressed (pro-B through late plasmablast); the most-used target in rheumatology (blinatumomab).
- CD20 — narrower (pre-B to early plasmablast); mosunetuzumab.
- BCMA — a TNF-receptor family member (ligands BAFF/APRIL) on late B cells, plasmablasts, and long-lived plasma cells — precisely the compartment where CD19 is downregulated. Teclistamab targets this, reaching antibody-secreting cells that anti-CD19/20 agents miss.
The Evidence Base (Small, Early, Heterogeneous)
- 12 studies, 80 patients: 33 SLE, 22 RA, 14 SSc, 6 IIM, 2 PSS, 3 other.
- Agents: 32 blinatumomab, 16 teclistamab, 15 mosunetuzumab, 17 other.
- Much of this is case reports and conference abstracts with short follow-up — findings are hypothesis-generating, not practice-changing.
Efficacy Signals by Disease
- SLE: A refractory lupus-nephritis case on teclistamab went from SLEDAI 20 → 0 by week 6 (sustained), with UPCR, dsDNA and complement normalising. Mosunetuzumab (15 pts): most with high baseline activity achieved meaningful reductions. A trispecific CD19 agent: all 5 patients achieved SRI-4, all 4 with LN improved proteinuria. A-319 (CD19 BiTE): 9/12 SRI-4.
- SSc: Consistent skin improvement — mRSS fell (e.g. 39→24; 36→21; median −10; 21→10). Lung function improved in several (FVC normalisation, regression of inflammation/fibrosis on CT/FAPI-PET). Anti-Scl-70 response was mixed (seroconversion in some, only partial reduction or no change in others).
- RA: DAS28-CRP fell into remission range (e.g. 5.9→1.9; mean 4.72→2.28 at 3 months), with drops in RF and anti-CCP. But durability was poor: in the 14-patient blinatumomab series, 9 reached remission at 3 months yet only one stayed in remission beyond that without adding a DMARD.
- IIM / anti-synthetase: Improvements in skin (CDASI), strength (MMT8), and enzymes; blinatumomab produced glucocorticoid-free remission in anti-synthetase syndrome (with rituximab maintenance).
- PSS: ESSDAI 34 → 12, but relapse at 5 months requiring retreatment; remission at 1 year.
Safety
- CRS in 46% — but overwhelmingly low-grade (33% G1, 12% G2, only 1% G3; no G4). All resolved; ~10 patients needed tocilizumab.
- No ICANS / neurotoxicity, no deaths reported — a notable and reassuring contrast to some CAR-T experience.
- Teclistamab drove far more CRS than blinatumomab (75% vs 28%), consistent with oncology data.
- Infections 35% (severe in 4%); hypogammaglobulinaemia 16%; haematologic toxicity 18% (all transient/low-grade).
- Overall CRS burden is similar to CAR-T in SLE.
The Central Tension — Dosing and Durability
This is the review’s most important and least obvious message. Rheumatology has been giving much less drug than oncology, on the assumption that a lower B-cell burden needs less:
- Blinatumomab: TOWER (B-ALL) delivers ~3,136 µg over 6 months; the rheumatology studies used 18–93 µg.
- In Tur et al.’s lymph-node biopsy comparison, CD19 CAR-T achieved complete nodal B-cell depletion with disrupted follicular architecture, whereas blinatumomab and rituximab gave only modest, incomplete tissue depletion — and the blinatumomab patients had received roughly half the TOWER cumulative dose.
- Circulating B cells deplete within 1–4 weeks, but reconstitute variably; each blinatumomab dose depleted less durably than assumed, and depletion was dose-dependent for mosunetuzumab.
The likely implication: TCEs are not “one-and-done” like CAR-T — they probably require repeated, sustained dosing to hold both circulating and tissue B cells down. Current under-dosing may explain the frequent post-treatment relapses (most visibly in RA).
Key Takeaways
- TCEs redirect the patient’s own T cells against autoreactive B/plasma cells — an off-the-shelf, repeatable, dose-adjustable alternative to CAR-T that could broaden access.
- Early efficacy is real but preliminary — rapid falls in disease activity, organ-specific improvement (renal in SLE, skin and lung in SSc, joints in RA), and serologic normalisation, across only 80 patients with short follow-up.
- Target choice maps to biology: CD19 (broad B-lineage), CD20 (narrower), and BCMA (reaches the plasma-cell compartment CD19/20 agents miss).
- Structure dictates practicality: Fv-based agents (blinatumomab) need continuous infusion; IgG-based agents (teclistamab) allow subcutaneous, less-frequent dosing but carry more Fc-related CRS.
- Safety looks manageable so far: CRS is common but mostly grade 1–2, with no neurotoxicity or deaths reported; teclistamab is more CRS-prone than blinatumomab.
- Durability is the weak point — relapse after discontinuation is frequent, best illustrated in RA, where remission rarely persisted past three months without added therapy.
- The dosing gap is the headline problem: rheumatology regimens deliver a small fraction of oncology exposure and give incomplete tissue B-cell depletion. Under-dosing — not lack of efficacy — may be driving recurrence.
- What’s needed next: prospective trials to define target antigens, dosing intensity/frequency/duration, long-term safety (infection, hypogammaglobulinaemia, cumulative immunosuppression), and head-to-head positioning against CAR-T and monoclonal antibodies.