TL;DR: In the TELIGAN phase 3 trial, once-weekly subcutaneous telitacicept reduced 24-h proteinuria by 55% relative to placebo over 39 weeks in high-risk IgA nephropathy — with eGFR essentially stable on treatment while declining on placebo — extending the BAFF/APRIL axis into a nephrology indication driven by the same B-cell biology familiar from SLE and RA.
The Clinical Problem
IgA nephropathy (IgAN) is the most common primary glomerulonephritis worldwide and a leading cause of kidney failure in young adults. Even with optimal supportive care, prognosis is sobering — median kidney survival to end-stage kidney disease is roughly 11 years in China and 12 years in the UK.
The pathogenesis is a well-described “multihit” cascade: production of galactose-deficient IgA1 (Gd-IgA1) → generation of anti-glycan autoantibodies → formation of circulating immune complexes → mesangial deposition → complement activation → mesangial proliferation → progressive glomerulosclerosis, tubulointerstitial fibrosis, and GFR loss.
For rheumatologists, the relevant link is upstream: B-cell homeostasis and IgA production are governed by two TNF-superfamily cytokines — BAFF (B-cell activating factor) and APRIL (a proliferation-inducing ligand). Both are elevated in IgAN and correlate with disease severity, making this axis a rational disease-modifying target rather than a purely symptomatic one.
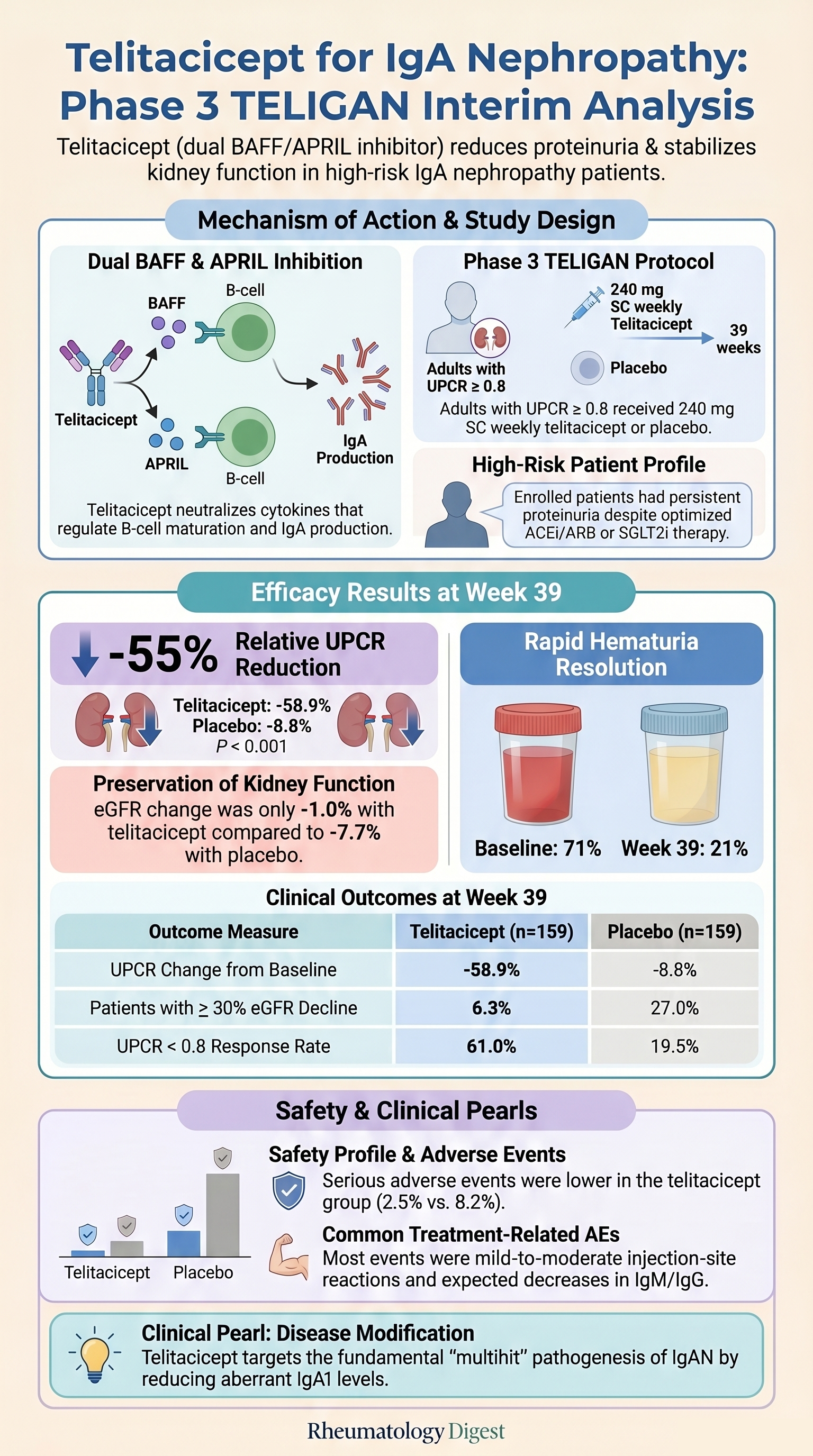
Telitacicept is a recombinant fusion protein combining the extracellular domain of the TACI receptor with the Fc domain of human IgG1. By acting as a TACI decoy, it simultaneously neutralises both BAFF and APRIL — distinguishing it from single-target agents. It is already approved in China for SLE, rheumatoid arthritis, and generalised myasthenia gravis. A prior phase 2 study showed proteinuria reduction and a fall in Gd-IgA1, providing the rationale for this phase 3 trial.
The Research Question
In adults with biopsy-proven IgAN and persistent proteinuria despite maximised supportive care, does 39 weeks of once-weekly subcutaneous telitacicept (240 mg) reduce proteinuria more than placebo?
How the Study Was Designed
The TELIGAN trial (NCT05799287) was a phase 3, multicentre (72 Chinese sites), double-blind, randomised, placebo-controlled study with a two-stage structure: Stage A reported here uses a 39-week proteinuria endpoint; Stage B is ongoing up to 104 weeks assessing eGFR slope.
Key inclusion criteria: biopsy-proven primary IgAN, age ≥18, persistent UPCR ≥0.8 g/g or 24-h urinary protein ≥1.0 g/day, eGFR ≥30 ml/min/1.73 m², and stable maximum-tolerated ACE inhibitor or ARB for ≥4 weeks. SGLT2 inhibitors were permitted; glucocorticoids and other immunosuppressants were prohibited (≥12-week washout).
Patients were randomised 1:1, stratified by baseline proteinuria, eGFR, and SGLT2i use. The primary endpoint was the geometric mean ratio (GMR) of 24-h UPCR at week 39 vs baseline, analysed by MMRM on the log scale. Stage A was powered at >90% (two-sided α 0.04) with 100 patients/group to detect an ~50% relative difference. Multiplicity adjustment applied to the primary endpoint only — all secondary confidence intervals are descriptive.
The Results
Population: 513 screened → 318 randomised (159 per arm). Completion was high (96.9% telitacicept, 94.3% placebo). Mean age 38.2 years, 53.8% women, mean baseline eGFR 75.5 ml/min/1.73 m², median UPCR ~1.26. All patients were on an ACE inhibitor/ARB; ~35% were on an SGLT2 inhibitor. Groups were well balanced including MEST-C histology.
Primary endpoint — proteinuria: Adjusted GMR of UPCR at week 39 was 0.41 (95% CI 0.37–0.46) with telitacicept vs 0.91 (0.81–1.02) with placebo — a percentage change of −58.9% vs −8.8%, and a relative difference of −55.0% (95% CI −61.3 to −47.6; P<0.001). Separation from placebo was visible by week 4 and widened progressively. Proteinuria response (UPCR <0.8) was achieved by 61.0% vs 19.5%.
Kidney function (secondary, descriptive): GMR of eGFR was 0.99 (0.97–1.01) vs 0.92 (0.90–0.95) — i.e. −1.0% vs −7.7%. Confirmed eGFR decline ≥30% occurred in 6.3% vs 27.0%.
Pharmacodynamic signals: Circulating CD19+ B cells fell by 46.4% (vs +4.5% with placebo). Mean serum IgA fell by 60.6% — biologically coherent given IgA1’s central pathogenic role. Haematuria (post-hoc, exploratory) fell from 71% to 21% with telitacicept; unchanged with placebo.
Safety: Any adverse event occurred in 89.3% vs 78.6%; treatment-related AEs in 77.4% vs 48.4%. Most events were mild–moderate — the excess was largely injection-site reactions (50.3% vs 13.8%) and expected immunoglobulin reductions (decreased IgM 24.5%, decreased IgG 13.2%). Serious adverse events were lower with telitacicept: 2.5% (n=4) vs 8.2% (n=13), with no treatment-related SAE in the telitacicept group. No patient had IgG fall below 3 g/L. No deaths in either arm. Among 68 patients with latent HBV, 0 of 31 on telitacicept had HBV DNA reactivation over 39 weeks.
Study Limitations
This is interim, surrogate-based data — Stage A used a 39-week proteinuria endpoint. The eGFR data are promising but descriptive, unadjusted for multiplicity, and await confirmation from the week-104 eGFR slope analysis in Stage B. The trial enrolled exclusively at Chinese sites; generalisability to European/North American populations is uncertain, though progression rates resembled the multinational TESTING trial. Sponsor (RemeGen) involvement in trial design, data collection, and adverse-event reporting is a standard caveat. Haematuria reduction was non-prespecified and exploratory. Long-term consequences of sustained BAFF/APRIL blockade — particularly infection risk and vaccine responses — need longer follow-up.
How This Study Adds to Practice
This provides phase 3 evidence that dual BAFF/APRIL blockade meaningfully reduces proteinuria in high-risk IgAN, on top of optimised RAS blockade and SGLT2 inhibition. The magnitude of reduction is broadly comparable to other emerging IgAN therapies — nefecon, sparsentan, atrasentan, iptacopan, and sibeprenlimab — and consistent with other TACI-Fc agents (povetacicept, atacicept), though direct cross-trial comparison is not valid.
For rheumatologists, this extends the clinical footprint of an agent already familiar from SLE, RA, and myasthenia gravis into a nephrology indication driven by the same B-cell biology — a useful conceptual bridge when teaching the BAFF/APRIL axis. The preliminary latent-HBV safety signal is practically relevant for B-cell–targeted therapy in HBV-endemic regions.
Final Takeaways
- In high-risk IgAN, telitacicept 240 mg weekly for 39 weeks reduced 24-h UPCR by 55% relative to placebo (P<0.001), with the effect emerging within 4 weeks.
- eGFR remained essentially stable on telitacicept while declining on placebo — promising, but a descriptive secondary finding awaiting week-104 confirmation.
- The safety profile was manageable and consistent with the drug class: more injection-site reactions and expected immunoglobulin lowering, but fewer serious adverse events than placebo and no deaths.
- This is interim data on a surrogate endpoint — durable kidney-function benefit, infection risk over time, and generalisability beyond Asian populations remain to be established.