TL;DR: In the first placebo-controlled RCT of a TLR7/8 inhibitor in lupus, the oral agent enpatoran met its primary endpoint with a dose-dependent reduction in cutaneous disease activity at 16 weeks — but the headline is mechanistic: it rapidly and reversibly switched off the skin interferon signature, pinning TLR7/8 as an upstream driver of cutaneous IFN activation. Steroid-sparing was not demonstrated, and the three doses could not be separated.
The Clinical Problem
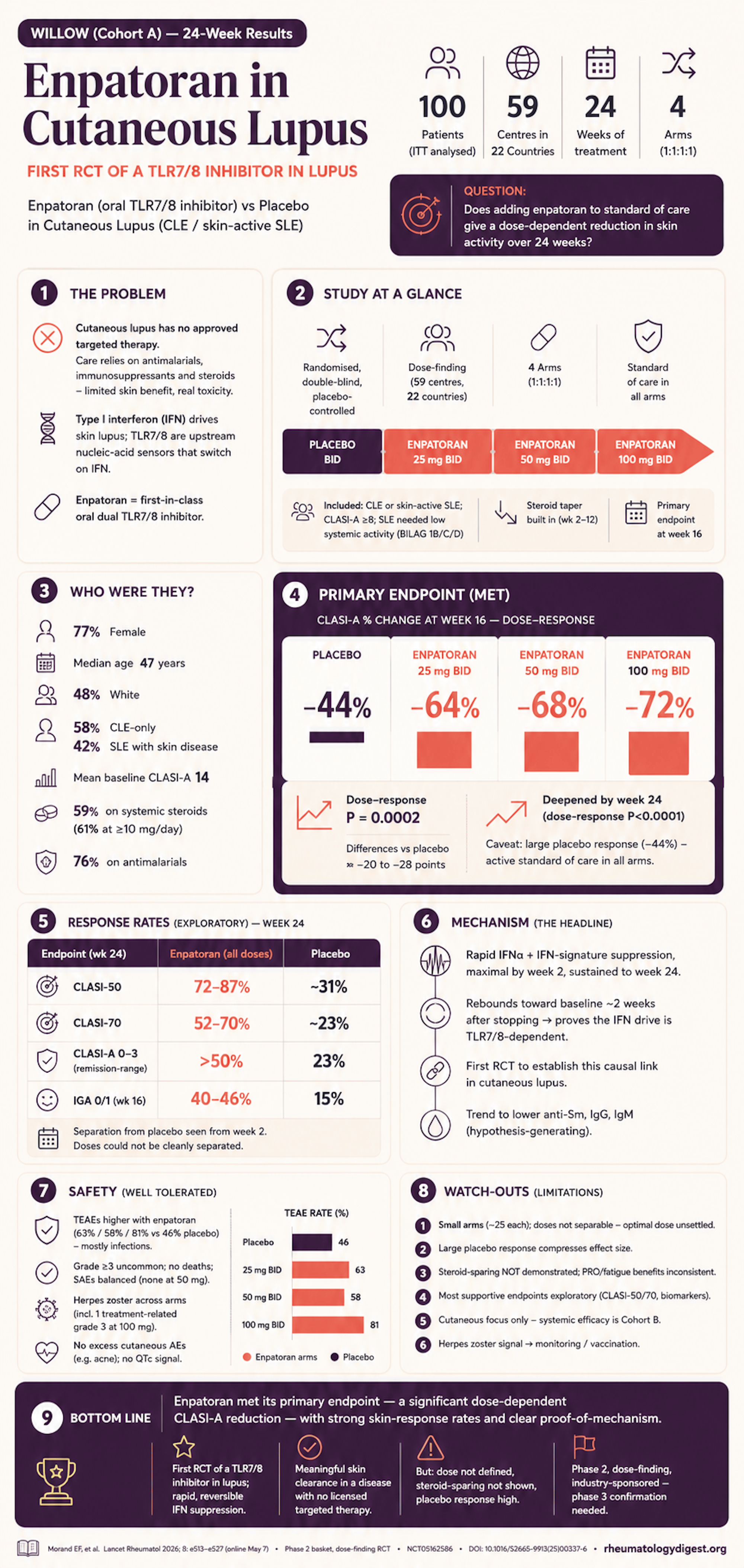
Cutaneous lupus erythematosus (CLE) — whether standalone or as a skin manifestation of SLE — carries a heavy quality-of-life burden, yet there is no approved targeted therapy for it. Current care leans on antimalarials, conventional immunosuppressants, some biologics (anti-CD20, anti-IFN receptor, anti-BAFF), and topical/systemic steroids, all of which give limited cutaneous benefit and meaningful toxicity. Chronic glucocorticoid exposure in particular drives irreversible organ damage, so steroid minimisation is a central goal.
Mechanistically, skin is an early and active site in lupus. Type I interferon (IFN) overexpression in lesional — and even non-lesional — skin is implicated in CLE, and cutaneous IFN activation may help trigger the autoantibody production and systemic inflammation of SLE. The upstream driver of this IFN surge has been uncertain. Toll-like receptors 7 and 8 (TLR7/8) are endosomal nucleic-acid sensors that can be triggered by endogenous nucleic acids, activating type I IFN and B lymphocytes — making them a rational, but until now clinically untested, target.
Enpatoran is a first-in-class oral small-molecule dual TLR7/8 inhibitor. Targeting both receptors (which differ in expression and function) is postulated to outperform blocking either alone. Earlier phase 1/1b work showed it was well tolerated, suppressed the IFN gene signature dose-dependently, and gave numerically greater disease-activity reductions than placebo.
The Research Question
In adults with active cutaneous lupus (CLE only, or SLE with skin involvement but low systemic activity), does adding enpatoran to standard of care produce a dose-dependent reduction in cutaneous disease activity over 24 weeks — and is it safe and well tolerated? The trial was explicitly a dose-finding study, so the primary question was about the dose–response relationship, not simply “drug vs placebo.”
How the Study Was Designed
Population (59 Cohort A centres across 22 countries; May 2022 – Feb 2024)
- Adults 18–75 years, CLE and/or SLE with cutaneous disease, symptom duration ≥6 months.
- CLASI-A ≥8 (active skin disease); documented active subacute CLE or discoid LE, biopsy- or photography-confirmed.
- SLE patients required low/no systemic activity (BILAG-2004 score 1B, C, or D).
- Stable background antimalarial/immunomodulator/immunosuppressant and/or steroid required.
- Excluded: another primary systemic autoimmune disease, drug-induced lupus, active lupus nephritis.
Randomisation & masking (1:1:1:1, double-blind)
- Standard of care plus placebo, or enpatoran 25 mg, 50 mg, or 100 mg twice daily for 24 weeks.
- Stratified by region and diagnosis (CLE/DLE vs SLE); participants, investigators, and sponsor masked.
- Design detail that matters: from weeks 2–12, glucocorticoids were tapered to ≤5 mg/day prednisone-equivalent as tolerated — a built-in steroid-reduction pressure applied to all arms.
Endpoints
- Primary: the dose–response relationship for percentage change from baseline in CLASI-A at week 16 (CLASI-A ranges 0–70; higher = worse), analysed by a multiple comparison procedure–modelling (MCP-Mod) approach.
- Prespecified exploratory CLASI-A: week-24 change, CLASI-50 and CLASI-70 responses, and remission thresholds (CLASI-A 0–1 and 0–3).
- Secondary: CLA-IGA, Physician Global Assessment, Skindex-29+3, FACIT-Fatigue, and clinically meaningful steroid reduction (≥10 mg to ≤5 mg by week 12, sustained to week 24).
- Biomarkers (exploratory): serum IFNα and whole-blood type I IFN gene signature (IFN-GS); autoantibodies (anti-Sm, Ro/SSA, La/SSB) and immunoglobulins.
Statistics
- 100 participants (25/group) gave ~80% power to detect the dose response, one-sided α=0.025, assuming a maximum placebo difference of −28% and SD 35%.
- Efficacy in the full analysis set (ITT); MCP-Mod for dose response; MMRM for supportive continuous analyses; Dunnett-adjusted CIs.
- Conservative handling: early discontinuation, protocol-prohibited medication changes, or non-compliant steroid use were all counted as non-response.
The Results
Who was studied
- 102 randomised, 100 analysed for efficacy (2 excluded post-randomisation for ineligible BILAG scores): placebo 26, enpatoran 25 mg 23, 50 mg 25, 100 mg 26. 94% completed 24 weeks.
- Median age 47 y; 77% female; 48% White (with meaningful Asian and Hispanic/Latino representation).
- 58% CLE-only, 42% SLE with cutaneous disease; mean baseline CLASI-A 14.0; ~71% had CLASI-A 10–70.
- 59% on systemic steroids at baseline (of whom 61% at ≥10 mg/day); 76% on antimalarials.
Primary endpoint — met
- A statistically significant, log-linear dose–response was confirmed (one-sided p=0.0002).
- Adjusted mean CLASI-A change at week 16: −64% (25 mg), −68% (50 mg), −72% (100 mg) vs −44% with placebo; differences vs placebo of roughly −20 to −28 percentage points.
- Key nuance: the placebo response was large (−44%) — expected in CLE trials where all patients receive active standard of care — so the incremental enpatoran effect, while real and consistent, sits on top of a high background response.
Week 24 and response rates (exploratory)
- The separation widened by week 24 (dose-response p<0.0001): CLASI-A change −69% / −74% / −79% vs −43% placebo.
- CLASI-50: 72–87% across enpatoran doses (overall effect p=0.0012); CLASI-70: 52–70% (p=0.0063) — both consistently above placebo from week 2 onward.
- Remission-range skin scores by week 24: >50% reached CLASI-A 0–3, and ~30% reached the stricter 0–1 (noting no validated CLE remission definition exists).
- Counterintuitive detail: the highest clinical response was not always at the highest dose (e.g., CLASI-50 at week 24 was numerically highest with 25 mg, 87%), and the MCP-Mod model could not cleanly separate the three doses from one another.
Supportive clinician and patient outcomes
- CLA-IGA 0/1 (clear/almost clear) at week 16: 43% / 40% / 46% vs 15% placebo (all ORs >4; p<0.025).
- PGA improved across doses. PRO signals were less consistent: Skindex-29+3 symptom domain improved with 25/50 mg; FACIT-Fatigue reached significance only at 50 mg; Worst-Itch NRS showed the clearest patient-reported benefit.
Mechanism — the biomarker story
- Enpatoran produced rapid, marked suppression of serum IFNα and IFN-GS, maximal by week 2 and maintained to week 24.
- Crucially, IFN-GS returned toward baseline ~2 weeks after stopping (week 26) — direct evidence that the endogenous IFN drive in cutaneous lupus is TLR7/8-dependent. This is the first RCT to demonstrate this causal link.
- A trend to lower anti-Sm, IgG, and IgM hints at an effect on the antibody-mediated axis (hypothesis-generating).
Steroid-sparing — a negative
- Among patients on ≥10 mg/day at baseline, there was no significant difference between enpatoran and placebo in achieving clinically meaningful steroid reduction. The steroid-sparing promise was not demonstrated in this cohort.
Safety — well tolerated
- TEAEs were more frequent with enpatoran (63% / 58% / 81% for 25/50/100 mg vs 46% placebo), driven mainly by infections (URTI most common). Grade ≥3 events were uncommon and balanced.
- Serious AEs: placebo 1, 25 mg 2, 100 mg 1, none at 50 mg; no deaths.
- Herpes zoster occurred across enpatoran arms (1 at 25 mg, 1 at 50 mg, 2 at 100 mg) — including one treatment-related grade 3 dermatomal case at 100 mg that resolved in 8 days.
- Reassuringly, no excess cutaneous AEs (e.g., acne) as seen with some other innate-immune agents, and no QTcF or ECG signal.
Study Limitations
- Small per-arm numbers (~25 each) limit precision, especially for response-rate and subgroup estimates.
- The dose–response model could not differentiate the three doses — so an optimal dose is not yet defined; exposure–response modelling (with Cohort B) is pending.
- Large placebo response (active standard of care + steroid taper) compresses the apparent treatment effect and complicates interpretation.
- Steroid-sparing endpoint not met, and PRO/fatigue benefits were inconsistent across doses.
- Mostly exploratory supportive endpoints (CLASI-50/70, biomarkers, PROs), so those results reinforce but cannot independently confirm efficacy.
- ~Half of participants were White, with under-representation of some groups — typical of lupus trials but relevant to generalisability.
- Cutaneous focus only: efficacy in antibody-mediated/systemic manifestations is addressed by Cohort B, not here; herpes zoster warrants monitoring and vaccination consideration.
How This Study Adds to Practice
- This is the first placebo-controlled RCT of a TLR7/8 inhibitor in lupus, and it delivers proof-of-mechanism: blocking TLR7/8 rapidly switches off the cutaneous IFN signature, and that signature rebounds on drug cessation — pinning TLR7/8 as an upstream driver of the IFN pathway in skin lupus.
- It provides randomised evidence of clinically meaningful skin improvement (CLASI-A, CLASI-50/70, IGA clear/almost-clear) in a disease with no licensed targeted therapy — a genuine unmet need.
- It complements the broader IFN-pathway story in lupus (anifrolumab, deucravacitinib, litifilimab), positioning oral TLR7/8 inhibition as a distinct, upstream strategy.
- Practically, it is hypothesis-defining rather than practice-changing: the drug is investigational, the optimal dose is unsettled, steroid-sparing was not shown, and confirmation requires phase 3 trials — which these data explicitly support.
Final Take-Aways
- Enpatoran met its primary endpoint — a significant dose-dependent reduction in CLASI-A at week 16 (−64% to −72% vs −44% placebo; p=0.0002) — with benefit emerging by week 2 and deepening to week 24.
- Response rates were strong (CLASI-50 up to ~87%, CLASI-70 up to ~70%), and >50% reached remission-range skin scores by week 24.
- The biomarker data are the headline: rapid, reversible IFNα/IFN-GS suppression confirms TLR7/8 as a driver of cutaneous IFN activation — a first in an RCT.
- Well tolerated, with an infection/herpes-zoster signal to watch and no cutaneous-AE or cardiac concern; steroid-sparing was not demonstrated.
- This is small, phase 2, dose-finding, industry-sponsored work that cannot yet separate the doses — a promising oral candidate for CLE that now needs phase 3 confirmation and dose refinement.